Anti-angiogenic combinations excel in later lines
VARGADO: nintedanib after immunotherapy
The ongoing, prospective, non-interventional VARGADO study is assessing the angiokinase inhibitor nintedanib plus docetaxel in patients with advanced adenocarcinoma of the lung after first-line chemotherapy in routine clinical practice. VARGADO is conducted at approximately 100 sites across Germany and includes 3 cohorts. Cohort A is receiving chemotherapy and nintedanib plus docetaxel in the first- and second-line settings, respectively; for Cohort B, immune checkpoint inhibition (ICI) constitutes the second-line treatment after chemotherapy and is followed by the nintedanib combination; in Cohort C, chemotherapy plus ICI treatment is administered in the first line and nintedanib plus docetaxel in the second line (Figure 1). At ELCC 2019, Grohé et al. presented the initial analysis of 22 patients included in Cohort B [1]. The results support the clinical benefit and manageable safety profile of nintedanib plus docetaxel in patients who have progressed after ICI treatment. Ten of 12 patients who responded achieved disease control (83 %), with PR occurring in 7 individuals (58 %) and SD in 3 (25 %). The observed clinical benefit of nintedanib plus docetaxel was consistent across responses and median PFS, which was 5.5 months. Also, the safety profile matched the known profile for the nintedanib combination. Drug-related treatment-emergent AEs comprised mainly stomatitis, decreased white blood cell counts, and nausea.
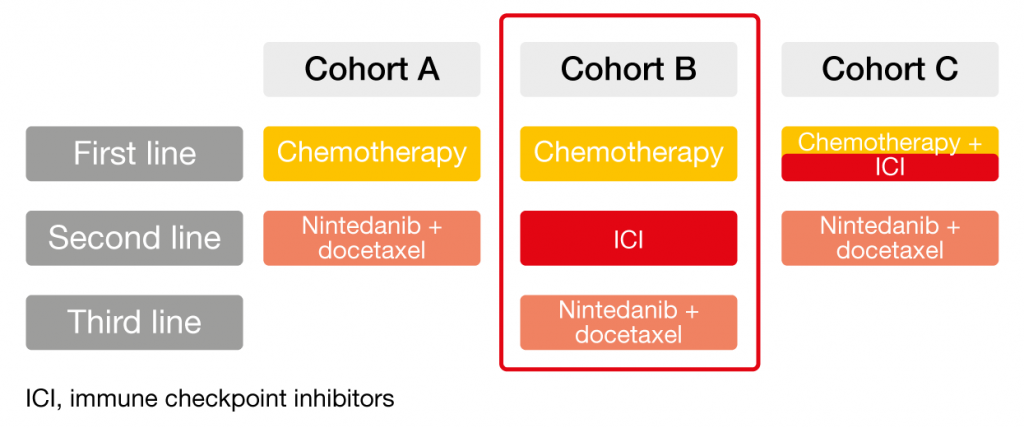
Figure 1: Design of the non-interventional VARGADO trial
Effects on the microenvironment
It was hypothesized that an angio-immunogenic switch might represent the underlying mechanism of the treatment activity observed in VARGADO. It has been shown that an immunosuppressive tumor microenvironment, which is closely linked to resistance to ICIs, is associated with VEGF-mediated angiogenesis [2]. Abnormal vasculature might contribute to ICI resistance. In this setting, anti-angiogenic therapy can support vessel normalization and improve access of immune cells to the tumor, tipping the balance towards an immunosupportive tumor microenvironment [3]. Targeting the microenvironment in this manner might reactivate and even enhance the effect of the ICI therapy. The authors noted that these initial data provide valuable clinical insights in an advanced lung cancer population for which only very little clinical evidence exists to date. VARGADO is ongoing, and patient recruitment has been expanded.
Bevacizumab plus EGFR TKIs
The combination of the anti-VEGF antibody bevacizumab with the first-generation EGFR TKI erlotinib has shown promising efficacy in the phase II JO25567 trial [4] and in the phase III NEJ026 study [5] that were performed in the first-line setting. However, the efficacy of EGFR TKI treatment plus bevacizumab in patients with EGFR-mutant NSCLC and brain metastases remains undetermined. Therefore, Jiang et al. conducted a multi-center, retrospective study to investigate whether the administration of the first-generation EGFR TKIs erlotinib, gefitinib and icotinib together with bevacizumab could improve survival compared to the TKIs alone in patients with multiple (i.e., > 3) brain metastases [6]. Overall, 208 patients with EGFR-mutant NSCLC and CNS disease were included in the analysis. Of these, 59 had been treated with a TKI and bevacizumab, while 149 had received TKI monotherapy. Erlotinib was the most commonly used EGFR TKI. Intracranial PFS, systemic PFS and OS were defined as the primary endpoints. For all of these outcomes, the combination brought about significantly superior results compared to TKI monotherapy. Median intracranial PFS was 14.0 months with bevacizumab plus TKI treatment versus 8.2 months with TKIs alone (HR, 0.56; p < 0.001); for systemic PFS, this was 14.4 vs. 9.0 months (HR, 0.55; p < 0.001). More importantly, the addition of bevacizumab led to a reduction in the mortality risk of almost 50 %, with median OS of 29.6 vs. 21.7 months (HR, 0.51; p < 0.001). Likewise, the combination group derived greater benefits regarding both intracranial responses (p = 0.001) and systemic responses (n = 0.019; Figure 2). Overall, these findings suggested that EGFR TKIs combined with bevacizumab are an option for patients with EGFR-mutant NSCLC and multiple brain metastases. This might even apply to the first-line setting, although prospective data are required here.
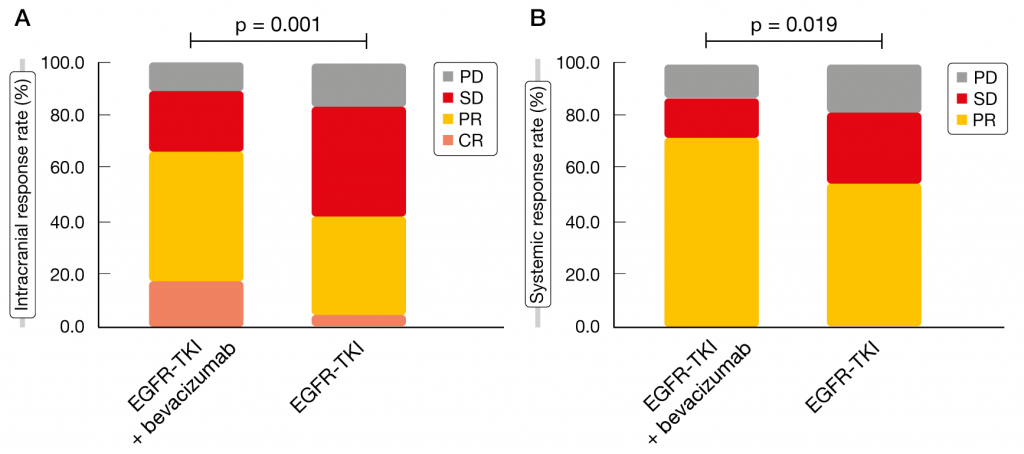
Figure 2: Intracranial (left) and systemic (right) responses with the addition of bevacizumab to EGFR TKI treatment compared to EGFR TKIs alone
REFERENCES
- Grohé C et al., Efficacy and safety of nintedanib plus docetaxel in lung adenocarcinoma patients following treatment with immune checkpoint inhibitors: first results of the ongoing non-interventional study VARGADO (NCT02392455). ELCC 2019, abstract 1190
- Fukumura D et al., Enhancing cancer immunotherapy using antiangiogenics: opportunities and challenges. Nat Rev Clin Oncol 2018; 15(5): 325-340
- van der Woude LL et al., Migrating into the tumor: a roadmap for T cells. Trends Cancer 2017; 3(11): 797-808
- Seto T et al., Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non-small-cell lung cancer harbouring EGFR mutations (JO25567): an open-label, randomised, multicentre, phase 2 study. Lancet Oncol 2014; 15(11): 1236-1244
- Naoki F et al., Phase III study comparing bevacizumab plus erlotinib to erlotinib in patients with untreated NSCLC harboring activating EGFR mutations: NEJ026. J Clin Oncol 36, 2018 (suppl; abstr 9006)
- Jiang T et al., EGFR TKIs plus bevacizumab demonstrated survival benefit than EGFR TKIs alone in EGFR-mutant NSCLC patients with multiple brain metastases. ELCC 2019, abstract 1890
More posts
Current perspectives in EGFR-targeted therapy
Current perspectives in EGFR-targeted therapy Global phase IIIb study assessing ...
Preface – ELCC 2019
Preface – ELCC 2019 Pilar Garrido, MD, PhD Head of the Thoracic Tumor Section, ...