Immune checkpoint blockade: determinants of treatment success
Various clinical factors beyond PD-L1 expression have been explored as predictors of response to immune checkpoint inhibition. Specifically, analyses have associated lack of tobacco exposure with diminished responsiveness to PD-1 pathway blockade in NSCLC [1, 2]. One possible explanation for this is that lung cancers arising in never or minimal smokers generally show low TMB [3]. As smoking exposure increases, the number of mutations per megabase rises as well. TMB has been established as an independent predictive biomarker of response to immune checkpoint inhibitors, with high TMB indicating more favourable responses [4, 5].
In their retrospective review, Gainor et al. explored the role of PD-(L)1 inhibition among never or light smokers with advanced NSCLC and high PD-L1 expression (TPS ≥ 50 %) [6]. This has not been well defined to date due to limited enrolment of never/light smokers in randomised studies and routine exclusion of certain molecular subsets (e.g., EGFR or ALK aberrations) in first-line clinical trials of PD-(L)1 inhibitors. Overall, 283 patients treated with checkpoint inhibitors from 4 institutions were evaluated; out of these, 69 were defined as never or light smokers, with 33 classified as never smokers (< 100 lifetime cigarettes) and 36 classified as light smokers (≤ 10 pack years; median number of pack years, 1.13). The majority of patients received PD-(L)1 inhibitors in the first-line setting.
Smoking habits influence DOR
The most common oncogenic driver mutations in never/light smokers included KRAS and EGFR mutations as well as MET exon 14 skipping. PD-L1 expression did not differ between never/light smokers and heavy smokers. TMB was assessed based upon smoking status; as expected, TMB was higher in heavy smokers (8.2 mut/Mb) than in never/light smokers (4.1 mut/Mb; p = 0.002), with median TMB being identical for never and light smokers.
In terms of anti-tumour activity of the anti-PD-(L)1 treatment, there was no statistically significant ORR difference between never/light smokers and heavy smokers (31.9 % vs. 39.6 %; p = 0.386). In 24 never smokers with measureable disease at baseline, the ORR was numerically lower at 25 %, although this was not statistically significant. Responses occurred across multiple oncogenic driver mutations, even though only 1 out of 8 patients with EGFR-mutant NSCLC responded (12.5 %), while this was the case for 4 out of 11 patients with KRAS-mutant disease (36.3 %). However, these results should be viewed cautiously, as the numbers of patients in this series were small. TMB did not affect responses to checkpoint inhibitors among never/light smokers. The PFS analysis showed a slight trend in favour of heavy smokers (4.8 vs. 3.29 months in never/light smokers; HR, 1.32; p = 0.105).
A conspicuous result, however, was the significant improvement in DOR observed with heavy smokers compared to never/light smokers (17.77 vs. 10.81 months; HR 4.32; p = 0.009; Figure 1) despite similar ORRs. The authors summarised that the immunobiological features determining initial response versus durability of response might be distinct. Given the shorter DOR with PD-(L)1 monotherapy, chemotherapy plus PD-1 combinations should be considered in never/light smokers with high PD-L1 expression.
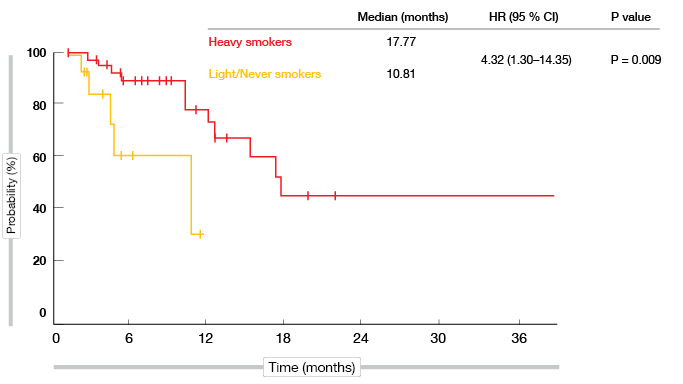
Figure 1: Significantly prolonged duration of response in heavy smokers versus light/never smokers
What does baseline steroid use do?
Corticosteroids are commonly employed in cancer care, as they can palliate and provide rapid relief of numerous cancer-related symptoms, and they are the mainstay of treatment for immune-related AEs. In this setting, steroids do not appear to diminish the activity of immune checkpoint blockade. However, the efficacy of PD-(L)1 inhibitors in patients receiving baseline steroids used to be unknown, as these patients were usually not eligible for clinical trials investigating immunotherapies.
Arbour et al. performed a retrospective review of the data of 455 and 185 patients from the Memorial Sloan Kettering Cancer Center (MSKCC) and the Gustave Roussy Cancer Center (GRCC), respectively, with the aim of evaluating the efficacy of PD-(L)1 inhibition in patients receiving baseline steroids (≥ 10 mg prednisone or equivalent on day 1 of treatment) [7]. At the two institutions, a total of 90 patients had been treated with steroids at the time of initiation of their PD-(L)1-inhibitory therapy.
Diminished activity in two independent cohorts
The data clearly demonstrated the deleterious effect of baseline steroid treatment on the PD-(L)1 blockade, such as lower ORR. In the MSKCC Cohort, complete and partial responses occurred in 6 % vs. 19 % in the steroid group and the group without steroids, respectively (p = 0.02). For the GRCC Cohort, the analysis revealed a similar distribution, with 8 % vs. 18 % (p = 0.2). Inferior PFS outcomes in patients receiving baseline steroids were observed in both cohorts (MSKCC: HR, 1.7; p < 0.0001; GRCC: HR, 1.5; p < 0.0001). Similarly, OS from the start of PD-(L)1 blockade therapy was significantly lower in the steroid groups at both institutions (MSKCC: HR, 2.1; p < 0.0001; GRCC: HR, 2.0; p < 0.001). Subgroup analyses using pooled data from both cohorts showed worse PFS and OS outcomes for patients receiving baseline steroids in nearly every subgroup. Of course, steroids are frequently used in a palliative setting for patients with brain metastases or poor performance status. According to a multivariate analysis, however, the deleterious PFS and OS effects of baseline steroid use remained after adjusting for negative prognostic variables.
The investigators pointed out that it is still uncertain whether the observed effect is predictive and/or prognostic. Based on these results, they recommended prudent use of steroids in patients for whom PD-(L)1 inhibition therapy is planned. This includes the consideration of non-steroid alternatives for the management of cancer symptoms, whereas medically necessary steroids (e.g., for the treatment of brain metastases) should not be withheld. As this analysis only incorporated patients on single-agent PD-(L)1 inhibition, the implications for those receiving chemotherapy and combinations with checkpoint inhibitors are uncertain.
Features predicting long-term response
Responses obtained with anti-PD-(L)1 therapy may last years in selected cases, but the features predicting long-term response (LTR) have not been described yet. Therefore, Rizvi et al. analysed 766 patients with advanced NSCLC who received anti-PD-(L)1 therapy at the MSKCC from 2011 through 2016 [8]. LTR was defined as PFS lasting longer than 18 months. This was true for 62 patients (8 % of the total cohort). Of these, 47 (76 %) achieved complete or partial responses, and 15 (24 %) achieved disease stabilisation. At the time of the analysis, 68 % remained progression-free.
The authors identified several features typical of LTR. Long-term responders had significantly higher TMB that those without LTR (12.24 vs. 6.34 mut/Mb; p < 0.001), and the proportion of patients with high PD-L1 expression was greater (p = 0.02; Figure 2). Moreover, ever-smokers constituted the vast majority of those with LTR, whereas never-smokers were the exception; for patients without LTR, this distribution was more balanced. The analysis yielded a significant difference between the two groups in this respect (p = 0.03). EGFR mutation status showed a negative association with LTR: none of the long-term responders carried an EGFR mutation, while this was the case for 12 % of patients without LTR (p = 0.002).
The direct comparison of long-term and short-term responders revealed that TMB, but not PD-L1 expression differed significantly between the two groups. Also, it was shown that the depth of response correlated with LTR, but not tumour burden. Baseline tumour burden was similar in long-term and short-term responders.
The authors concluded that the features predicting durable response might indeed be distinct from the features predicting initial response on which biomarkers usually focus.
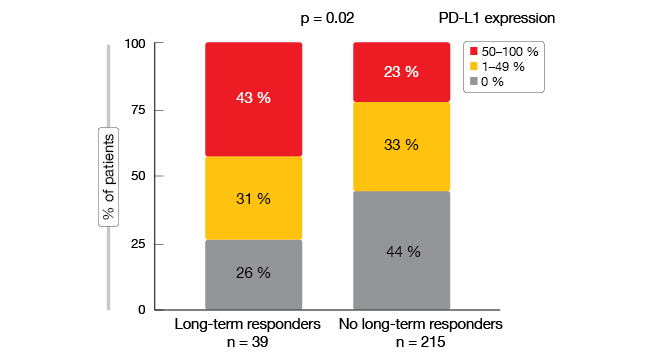
Figure 2: Greater proportion of high PD-L1 expression in patients with LTR
REFERENCES
- Borghaei H et al., Nivolumab versus docetaxel in advanced non-squamous non-small cell lung cancer. N Engl J Med 2015; 373(17): 1627-1639
- Gainor JF et al., EGFR mutations and ALK rearrangements are associated with low response rates to PD-1 pathway blockade in non-small cell lung cancer: a retrospective analysis. Clin Cancer Res 2016; 22(18): 4585-4593
- Gibbons DL et al., Smoking, p53 mutation, and lung cancer. Mol Cancer Res 2014; 12(1): 3-13
- Rizvi H et al., Molecular determinants of response to anti-programmed cell death (PD)-1 and anti-programmed death-ligand 1 (PD-L1) blockade in patients with non-small-cell lung cancer profiled with targeted next-generation sequencing. J Clin Oncol 2018; 36(7): 633-641
- Hellmann M et al., Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N Engl J Med 2018; 378(22): 2093-2104
- Gainor JF et al., Response and durability of checkpoint blockade in never- or light-smokers with NSCLC and high PD-L1 expression. J Clin Oncol 36, 2018 (suppl; abstr 9011)
- Arbour KC et al., Deleterious effect of baseline steroids on efficacy of PD-(L)1 blockade in patients with non-small cell lung cancer. J Clin Oncol 36, 2018 (suppl; abstr 9003)
- Rizvi H et al., Clinical and molecular features predicting long-term response (LTR) to anti-PD-(L)1 based therapy in patients with NSCLC. J Clin Oncol 36, 2018 (suppl; abstr 9022)
More posts
Comprehensive sequencing of plasma cell-free DNA permits non-invasive cancer detection
Early detection of lung cancer is a highly unmet medical need. Even though low-dose computed tomography (LDCT) has been shown to improve lung cancer mortality in high-risk individuals, the rate of clinical adoption remains low at 1.9 %. Cell-free DNA (cfDNA) testing might substitute LDCT as a screening tool, according to preliminary results of the Circulating Cell-free Genome Atlas (CCGA) Study presented at the ASCO Congress.
Recent benchmarks in the management of small-cell tumours
Extensive-disease small-cell lung cancer (ED-SCLC) is highly responsive to first-line therapy, but early relapses commonly occur, and prognosis is poor. To date, no biomarker-driven therapies have been established. Based on the involvement of the immune system in the pathophysiology of SCLC and the high mutational burden of this disease, immunotherapy has potential as a novel treatment option.
ALK-positive disease: pushing the borders of treatability
Standard treatment for patients with ALK-positive, advanced NSCLC includes the first-generation ALK inhibitor crizotinib and, more recently, second-generation ALK TKIs such as ceritinib and alectinib. The global, phase III ALEX trial tested the highly selective, CNS-active ALK inhibitor alectinib as first-line agent compared to crizotinib in patients with stage IIIB/IV ALK-positive NSCLC. Asymptomatic brain metastases were allowed in this study.
Interview with Barbara Melosky: “The sequencing question remains”
Afatinib has been licensed for the second-line treatment of patients with squamous-cell carcinoma of the lung. A combination trial is ongoing that is testing afatinib plus pembrolizumab. What can we expect from this regimen?
New data on EGFR-directed TKIs across 3 generations
EGFR TKI treatment has become a standard first-line strategy for patients with advanced, EGFR-mutation–positive NSCLC. Established agents include the first-generation drugs gefitinib and erlotinib, the second-generation agents afatinib and dacomitinib, and the third-generation TKI osimertinib. Combinations of EGFR TKIs with other drug classes might lead to outcome optimisation, for instance the additional administration of anti-angiogenic drugs, such as bevacizumab and ramucirumab.
Immune checkpoint blockade: determinants of treatment success
Various clinical factors beyond PD-L1 expression have been explored as predictors of response to immune checkpoint inhibition. Specifically, analyses have associated lack of tobacco exposure with diminished responsiveness to PD-1 pathway blockade in NSCLC. One possible explanation for this is that lung cancers arising in never or minimal smokers generally show low TMB.