Combinational immunotherapy of nivolumab and ipilimumab prolongs survival in comparison to standard chemotherapy in malignant pleural mesothelioma
CheckMate743, a randomized, open-label, phase III study evaluate the efficacy and safety of the combination treatment of two immunotherapy drugs, nivolumab (NIVO), an anti-PD-1 antibody, and ipilimumab (IPI), an anti-CTL4-A antibody, as compared to standard chemotherapy in patients with malignant pleural mesothelioma (MPM). Patients diagnosed with an unresectable MPM with no prior systemic therapy and good ECOG performance status (0 or 1) were enrolled in the trial. Tumor histology (epithelioid vs non-epithelioid) and gender were two factors used to stratify patients before randomization.
A total of 605 patients were randomized in a 1-to-1 ratio to receive either standard chemotherapy of cisplatin/carboplatin plus pemetrexed for six cycles or immunotherapy combination of NIVO every two weeks plus IPI every six weeks for up to 2 years or until disease progression or unacceptable toxicity. The primary endpoint for the study was overall survival (OS).
The baseline characteristics were similar between both treatment groups, with around 40% of patients belonging to the ECOG performance status 0, 40% never smokers and 75% categorized histologically as epithelioid. About 20% of patients had <1% PD‑L1 expression at baseline, quantified using a PD-L1 immunohistochemistry assay.
The data from a prespecified interim analysis of CheckMate743, after a median follow-up of 29.7 months, showed that the trial met its primary endpoint with the combination treatment of NIVO and IPI yielding a significant 4-month improvement in median OS as compared to platinum doublet chemotherapy (18.1 vs 14.1 months), after a median follow-up of 29.7 months (Figure 1).

Figure 1: Median Overall Survival (OS) as the primary endpoint of the CheckMate 743 study
The improvement in OS was consistent among almost all subgroups, especially in patients categorized with non-epithelioid tumor (Figure 2) and patients with PD-L1≥1% (Figure 3).

Figure 2: Median OS by tumor histology
Although the NIVO plus IPI treatment arm showed similar outcomes compared to the standard chemotherapy arm for other efficacy outcomes such as median progression-free survival (mPFS) (6.8 vs 7.2 months, HR 1.00, 95% 0.82 – 1.2) and the objective response rate (ORR) (40% vs 43%), the duration of response (DOR) different, with DOR of 11 months with NIVO plus IPI at 11 months vs 6.7 months with chemotherapy.
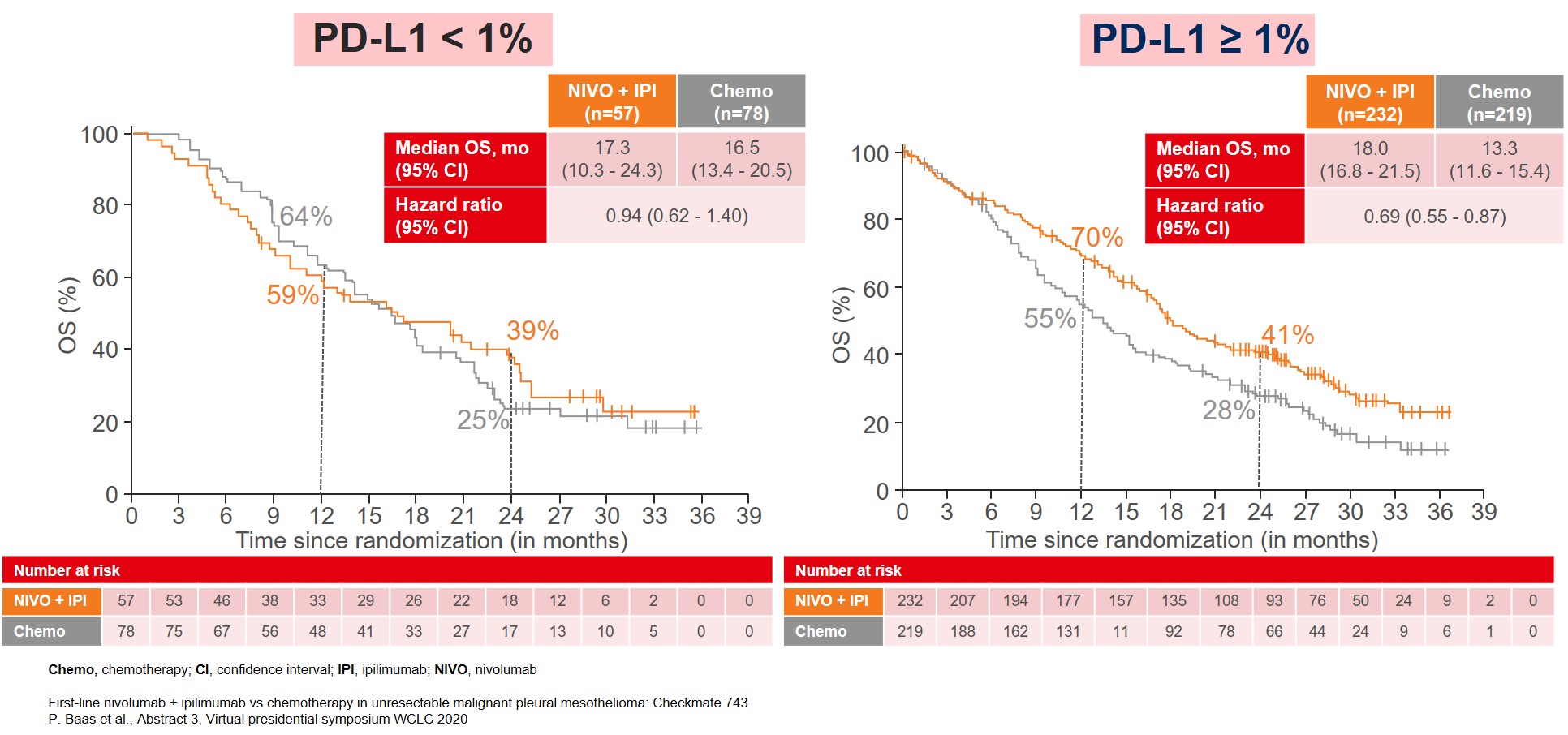
Figure 3: Median OS by PD-L1 expression
The adverse event profiles for the two treatment regimens were markedly different but consistent with the AEs previously seen at a similar dose and schedule in other studies with the most common treatment-related adverse events (TRAEs) (≥15%) in the NIVO plus IPI group being diarrhea and pruritis whereas with standard chemotherapy the most common TRAES were anemia, neutropenia, fatigue, decreased appetite and asthenia. The difference in the incidence of serious TRAEs (15% vs 6%) and TRAEs leading to discontinuation of treatment regimen (15% vs 7%) was higher in NIVO plus IPI group compared to chemotherapy.
In conclusion, the results reported from the CheckMate743 trial led to the approval of nivolumab and ipilimumab by the Food and Drug Administration as first-line treatment patients with all types of unresectable malignant pleural mesothelioma across all subgroups1.
REFERENCE
- https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-nivolumab-and-ipilimumab-unresectable-malignant-pleural-mesothelioma
More posts
Nivolumab as a new option in patients with relapsed malignant mesothelioma
Until recently, no randomized phase III trials have demonstrated OS improvement in patients with relapsed malignant mesothelioma. PD-1 inhibition with single-agent nivolumab has shown activity in three phase II studies, one of which led to the approval of nivolumab in Japan.
Interview: Lung cancer screening: hurdles in daily routine and in the research laboratory
All of us agree that LDCT is effective and should be widely implemented. I would say that cost and awareness are the two major issues that are impeding the implementation of LDCT all over the world. Cost-effectiveness of LDCT has been demonstrated by many publications; and there are even other arguments in favor of the cost-effectiveness of this technology.
Immunotherapy: combination regimens and new data on the significance of mutations
Substantial OS and PFS improvements have led to the implementation of the regimen evaluated in the KEYNOTE-189 trial as standard first-line approach for stage IV non-squamous NSCLC without sensitizing EGFR/ALK alterations.
What is new in SCLC?
A novel approach for targeting lung tumors with small-cell histology consists in the inhibition of transactivated transcription, as small-cell lung cancer (SCLC) has been found to be a transcription-addicted malignancy. Rudin et al. defined four molecular SCLC subtypes according to their differential expression of four key transcription regulators.
Interview: Antibody-drug conjugates: the age of almost unlimited possibilities has just begun
Antibody-drug conjugates have opened up an entirely new paradigm. Targeted therapy requires specific mutations, and immunotherapy only works if the tumor expresses neoantigens or is essentially able to respond to these agents. As we know, these two approaches do not work forever, not every patient responds to them, and certainly not every patient has a targetable mutation.
Specific treatment approaches in the EGFR-mutated setting
EGFR exon 20 insertion mutations are found in approximately 5 % to 12 % of EGFR-mutated NSCLC tumors, i.e., in 2 % of all NSCLC cases. They represent the third most common EGFR mutation after L858R and exon 19 deletion. However, EGFR TKIs cannot be used to treat lung cancer with exon 20 insertions as they are insensitive to these drugs due to steric hindrance at the TKI-binding site.