Distinct somatic genome variations in young lung cancer patients
Lung cancer in young adults is relatively rare, but it is considered a unique subgroup with distinct biology [1]. In patients aged ≤ 40 years, the incidence of lung cancer has been found to be 4 % [2], and in those aged ≤ 45 years, 5.3 % [3]. Characteristically, women are more often affected than men; adenocarcinoma prevails, and the stage of disease is frequently advanced at the time of the diagnosis. Of course, these patients usually receive aggressive treatment.
According to recent studies in young lung cancer patients, actionable genomic targets such as EGFR and ALK aberrations might be more enriched in this population [2]. There was also a trend with regard to HER2 and ROS1 alterations. Hsu et al. found no significant difference in survival between young lung cancer patients with and without EGFR mutation [4]. However, the broader genomic landscape and related oncogenic pathways are not fully understood yet.
Overlap with TCGA genes
Therefore, Wu et al. performed whole exome sequencing based upon paired normal blood DNA and formalin-fixed, paraffin-embedded genomic DNA in 27 Chinese NSCLC patients aged ≤ 45 years (median, 40; range, 31–45) [5]. Adenocarcinoma was present in 18 patients, and 21 were female. All of them had never smoked or did not smoke at the time of diagnosis. The investigators identified adenocarcinoma (AD) and squamous-cell carcinoma (SC) somatic variants, ending up with 288 and 151 AD and SC variants, respectively. Among genomic variant types, frameshift variants and missense variants predominated in both AD and SC (Figure). For both histologies, insertion or deletion polymorphisms (indels) were present in approximately 60 % and SNPs in approximately 40 %. The majority of mutated genes in both cohorts overlapped with the mutated genes obtained in the young NSCLC The Cancer Genome Atlas (TCGA) cohort for each disease subtype (i.e., 86 of 94 AD mutated genes and 41 of 48 SC mutated genes).
Genes with predicted high-impact mutations were selected for the pathway analysis, which yielded somatically altered candidate pathways that differed across histologies. For example, ERK/MAPK signaling and PTEN cell cycle arrest were altered in AD, but not in SC. Conversely, this was true for Trk/PI3K signaling and ADP ribosylation/DNA repair, among others, in SC, but not in AD. Further bioinformatic analyses are ongoing to compare the mutated genes and pathways in young patients with older TCGA cohorts.
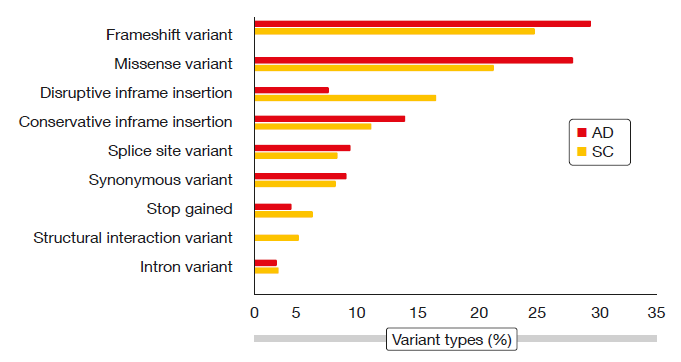
Figure: Genomic variant types in young patients with adenocarcinoma (AD) or squamous-cell
carcinoma (SC) of the lung
REFERENCES
- Luo W et al., Characteristics of genomic alter-ations of lung adenocarcinoma in young never-smokers. Int J Cancer 2018 Apr 18. doi: 10.1002/ijc.31542. [Epub ahead of print]
- Sacher AG et al., Association between younger age and targetable genomic alterations and prognosis in non-small-cell lung cancer. JAMA Oncol 2016; 2(3): 313-20
- Zhang J et al., Multicenter analysis of lung cancer patients younger than 45 years in Shang-hai. Cancer 2010; 116(15): 3656-3662
- Hsu CL et al., Advanced non-small cell lung cancer in patients aged 45 years or younger: outcomes and prognostic factors. BMC Cancer 2012; 2012 Jun 13; 12: 241
- Wu X et al., Whole exome sequencing (WES) to define the genomic landscape of young lung cancer patients (pts). J Clin Oncol 36, 2018 (suppl; abstr 12005)
More posts
Comprehensive sequencing of plasma cell-free DNA permits non-invasive cancer detection
Early detection of lung cancer is a highly unmet medical need. Even though low-dose computed tomography (LDCT) has been shown to improve lung cancer mortality in high-risk individuals, the rate of clinical adoption remains low at 1.9 %. Cell-free DNA (cfDNA) testing might substitute LDCT as a screening tool, according to preliminary results of the Circulating Cell-free Genome Atlas (CCGA) Study presented at the ASCO Congress.
Recent benchmarks in the management of small-cell tumours
Extensive-disease small-cell lung cancer (ED-SCLC) is highly responsive to first-line therapy, but early relapses commonly occur, and prognosis is poor. To date, no biomarker-driven therapies have been established. Based on the involvement of the immune system in the pathophysiology of SCLC and the high mutational burden of this disease, immunotherapy has potential as a novel treatment option.
ALK-positive disease: pushing the borders of treatability
Standard treatment for patients with ALK-positive, advanced NSCLC includes the first-generation ALK inhibitor crizotinib and, more recently, second-generation ALK TKIs such as ceritinib and alectinib. The global, phase III ALEX trial tested the highly selective, CNS-active ALK inhibitor alectinib as first-line agent compared to crizotinib in patients with stage IIIB/IV ALK-positive NSCLC. Asymptomatic brain metastases were allowed in this study.
Interview with Barbara Melosky: “The sequencing question remains”
Afatinib has been licensed for the second-line treatment of patients with squamous-cell carcinoma of the lung. A combination trial is ongoing that is testing afatinib plus pembrolizumab. What can we expect from this regimen?
New data on EGFR-directed TKIs across 3 generations
EGFR TKI treatment has become a standard first-line strategy for patients with advanced, EGFR-mutation–positive NSCLC. Established agents include the first-generation drugs gefitinib and erlotinib, the second-generation agents afatinib and dacomitinib, and the third-generation TKI osimertinib. Combinations of EGFR TKIs with other drug classes might lead to outcome optimisation, for instance the additional administration of anti-angiogenic drugs, such as bevacizumab and ramucirumab.
Immune checkpoint blockade: determinants of treatment success
Various clinical factors beyond PD-L1 expression have been explored as predictors of response to immune checkpoint inhibition. Specifically, analyses have associated lack of tobacco exposure with diminished responsiveness to PD-1 pathway blockade in NSCLC. One possible explanation for this is that lung cancers arising in never or minimal smokers generally show low TMB.