DUBLIN-3: microtubule-binding agent plinabulin in later lines
Patients with EGFR-wildtype, advanced NSCLC in the second or third treatment line represent a large population with limited treatment options. A novel approach is the first-in-class selective immunomodulating microtubule-binding agent (SIMBA) plinabulin that releases the immune defense protein GEF-H1, thus inducing dendritic cell maturation, which is a key step in the initiation of durable anti-cancer response [1, 2]. The global, randomized phase III DUBLIN-3 trial tested plinabulin 30 mg/m2 in addition to docetaxel Q3W (n = 278) versus docetaxel plus placebo (n = 281) in patients with non-squamous or squamous, stage IIIb/IV NSCLC who had progressed during or after one or two platinum-based regimens. Overall survival constituted the primary endpoint.
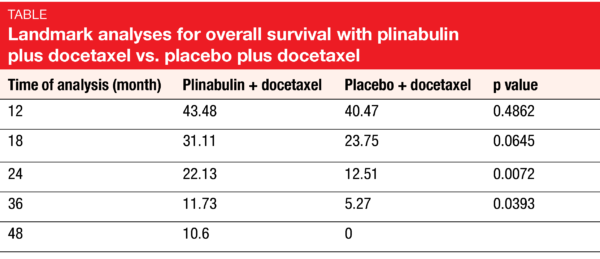
According to the results presented by Feinstein et al. at ESMO 2021, the DUBLIN-3 study met its primary objective [3]. Median OS was 10.5 vs. 9.4 months for plinabulin plus docetaxel vs. docetaxel alone (HR, 0.82; p = 0.0399). The combination gave rise to doubling of the OS rates at 24 and 36 months (Table). Likewise, the key secondary endpoints of DUBLIN-3 were met: median PFS was 3.6 vs. 3.0 months (HR, 0.76; p = 0.0082), with significantly higher PFS rates at 6 months (30.3 % vs. 17.8 %) and 12 months (17.1 % vs. 4.7 %). ORR was doubled with the addition of plinabulin (12.23 % vs. 6.76 %; p = 0.0275).
Durable activity and decreased grade 4 neutropenia
As the exploratory analysis demonstrated, the OS advantage was larger in the group that received ≥ 8 cycles (28.2 vs. 19.3 months; HR, 0.453; p = 0.0121) than in those treated with ≥ 4 cycles (18.3 vs. 13.5 months; HR, 0.634; p = 0.0022). Moreover, the analysis revealed a favorable long-term OS trend for the experimental regimen in the cohort that had been exposed to PD-(L)1-targeted therapy prior to study inclusion (i.e., 23 % of the total population), with 48-month OS rates of 12.5 % vs. 0 %. Pooled data from the phase IB/II 101 study and DUBLIN-3 suggested long-term survival benefit with the combination in Western patients.
Grade 3/4 AEs adjusted for cycle number per patient per year occurred less commonly in the experimental arm than in the control arm (estimated event rate, 9.88 vs. 11.04; p = 0.0253). Grade 4 neutropenia on day 8 in all cycles was significantly reduced with the combination (5.13 % vs. 33.58 %; p < 0.0001). Among non-hematological grade 3/4 AEs, diarrhea was reported more commonly for plinabulin plus docetaxel (8.4 % vs. 0.7 %), as was hypertension (17.2 % vs. 1.1 %) that transiently occurred after the infusion. According to the Q-TWiST analysis integrating efficacy, safety and quality of life, patients treated with the combination derived a > 18 % improvement, which is clinically meaningful. The authors concluded that plinabulin plus docetaxel shows a favorable risk-benefit ratio and has the potential of a preferred second/third-line treatment option in the setting of NSCLC with EGFR wildtype.
REFERENCES
- Kashyap AS et al., GEF-H1 signaling upon microtubule destabilization is required for dendritic cell activation and specific anti-tumor responses. Cell Rep 2019; 28(13): 3367-3380
- Singh AV et al., A novel vascular disrupting agent plinabulin triggers JNK-mediated apoptosis and inhibits angiogenesis in multiple myeloma cells. Blood 2011; 117(21): 5692-700
- Feinstein T et al., DUBLIN-3 (BPI-2358-103): a global phase 3 trial with the plinabulin/docetaxel combination vs. doc in 2nd/3rd line NSCLC patients with EGFR-wild type progressing on a prior platinum-based regimen. ESMO 2021, LBA48
© 2021 Springer-Verlag GmbH, Impressum
More posts
ATALANTE-1: anti-cancer vaccination after IO failure
OSE-2101 is an anti-cancer vaccine with modified neoepitopes restricted to HLA-A2+ targeting the tumor-associated antigens CEA, p53, HER2, MAGE-2 and MAGE-3 that are frequently expressed in lung cancer. HLA-A2 is assessed in the serum and is positive in approximately half of patients.
Gradual progress in the management of mesothelioma and thymoma
This is an important field where little progress has been made in the past. At ESMO 2021, updated results of the randomized CheckMate-743 trial of nivolumab plus ipilimumab versus chemotherapy were presented by Prof. Peters. The overall survival benefit was pronounced in patients with PD-L1–positive or non-epithelioid mesotheliomas, although there was an OS benefit in the total population.
Malignant pleural mesothelioma: immunotherapy-based approaches in all treatment lines
The randomized phase III CheckMate 743 trial evaluated nivolumab 3 mg/kg Q2W plus ipilimumab 1 mg/kg Q6W for up to 2 years compared with cisplatin or carboplatin plus pemetrexed Q3W for 6 cycles as first-line treatment of patients with unresectable malignant pleural mesothelioma (MPM). More than 300 patients were randomized into each study arm.
Small-cell lung cancer: on the road to improved efficacy and tolerability
Lurbinectedin, a selective inhibitor of oncogenic transcription, has been approved at a dose of 3.2 mg/m2 Q3W for the treatment of patients with small-cell lung cancer (SCLC) showing disease progression on or after platinum-based chemotherapy in the US. The randomized, phase III ATLANTIS trial tested the combination of lurbinectedin 2 mg/m2 and doxorubicin 40 mg/m2 Q3W for a maximum of 10 cycles followed by lurbinectedin 3.2 mg/m2 Q3W in 307 patients with relapsed SCLC after one prior chemotherapy line.
Immunotherapy: boosting efficacy and overcoming resistance
The global, randomized, open-label, phase III POSEIDON trial evaluated the PD-L1 inhibitor durvalumab with or without the anti-CTLA-4 antibody tremelimumab in addition to chemotherapy as a first-line strategy in the setting of metastatic NSCLC. At 153 sites in 19 countries, 1,013 patients with squamous or non-squamous, stage IV NSCLC were randomized into three arms.
Innovative and established agents across a range of targets
HER2 mutations constitute the predominant driver aberration in approximately 3 % of non-squamous NSCLC cases. While approved HER2-targeted therapies for patients with NSCLC are still lacking, the anti-HER2 antibody-drug conjugate trastuzumab deruxtecan (T-DXd) has been licensed in various countries for use in other HER2-positive entities.