Expansion of clinical trial enrollment criteria: what would we gain?
Broadened vs. traditional: retrospective analysis
In 2017, the American Society of Clinical Oncology and the non-profit organization Friends of Cancer Research noted in their joint statement that trial enrollment criteria should strive for inclusiveness to make trial populations more representative and to maximize generalizability of findings [1]. Also, this would enable more patients to participate and accelerate accrual, resulting in expedited availability of new therapies. Harvey et al. conducted a retrospective study using real-world data obtained between January 2011 and December 2018 to demonstrate the impact of broadened versus traditional criteria on the eligibility of patients with advanced NSCLC [2]. Based on the ASCO CancerLinQ Discovery (CLQD) deidentified electronic health record, patients who received treatment after a diagnosis of advanced NSCLC were identified. Outcome measures related to the number and characteristics of patients eligible by traditional vs. broadened criteria. Specifically, three domains of criteria were evaluated, i. e., prior and concurrent cancers, brain metastases, and kidney function. Patients with a cancer history, brain metastases and creatinine clearance ≤ 60 mL/min are usually excluded from clinical studies. According to the broadened criteria, all cases with another primary cancer diagnosis were included, as well as all patients with brain metastases irrespective of treatment status and clinical stability, and those with creatinine clearance ≥ 30 mL/min.
Doubling of eligible patients
Within the total group of 10,500 patients, according to the traditional criteria, the proportions of patients excluded due to prior/concurrent cancers, brain metastases, and creatinine clearance ≤ 60 mL/min were 21.5 %, 21.2 %, and 14.4 %, respectively. Overall, 47.7 % of these patients would not have been able to participate in clinical trials. The broadened criteria, on the other hand, only prompted exclusion of 1.5 % based on the creatinine clearance cut-off. Thus, the traditional and broadened cohorts comprised 5,495 and 10,346 patients, respectively, with the broadened cohort containing a comparably higher percentage of patients aged > 75 years (22.23 % vs. 16.09 %; Figure). This analysis shows that the use of expanded criteria would enable almost twice as many patients with advanced NSCLC to consider trial participation. Moreover, these criteria are likely to result in trial participants being more reflective of a broader patient population. The authors noted that narrower criteria should only be used based on a compelling scientific rationale. Additional recommendations by ASCO and Friends of Cancer Research are in progress.
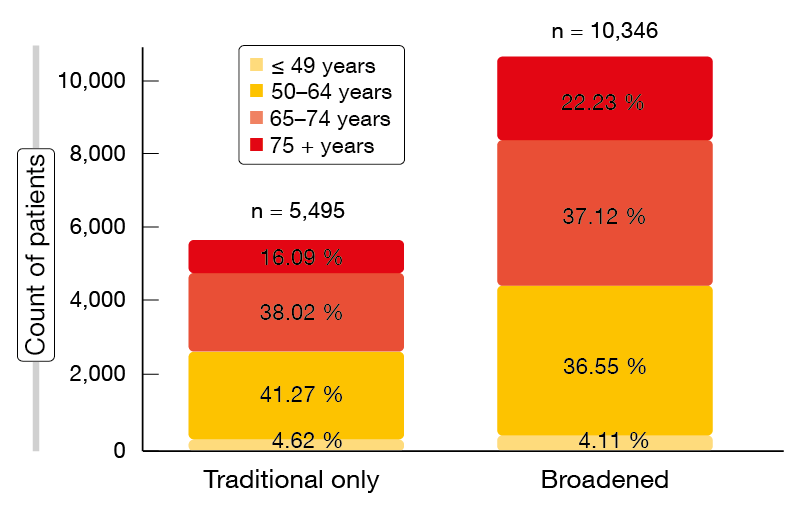
Figure: Distribution of age groups in the traditional and broadened cohorts
REFERENCES
- Kim ES et al., Broadening eligibility criteria to make clinical trials more representative: American Society of Clinical Oncology and Friends of Cancer Research Joint Research Statement. J Clin Oncol 2017; 35(33): 3737-3744
- Harvey RD et al., Impact of broadening clinical trial eligibility criteria for advanced non-small cell lung cancer patients: real-world analysis. J Clin Oncol 37, 2019 (suppl; abstr LBA108)
More posts
Small-cell tumors: improvements in the second-line setting
Only limited therapeutic options are available for patients with relapsing small-cell lung cancer (SCLC). Topotecan is the only FDA-approved treatment for platinum-sensitive disease in the second-line setting. However, it induces merely modest clinical benefits, while at the same time giving rise to significant hematological toxicity.
Rare mutations: taking treatment one step further
MET exon 14 skipping mutations (METex14) have been reported in 3 % to 4 % of NSCLC patients. They confer poor prognosis and poor responses to standard therapies including immunotherapy. Moreover, patients with MET alterations are generally older, which implies that tolerable strategies are called for. Capmatinib has been developed as a highly selective, potent MET inhibitor with in vitro and in vivo activity against preclinical cancer models harboring MET activation.
Interview: Blood-based testing in ALK-positive disease
What can we expect from circulating free DNA (cfDNA) as a biomarker in the setting of lung cancer diagnosis and treatment today?
Trial updates and new biomarkers in the field of immunotherapy
KEYNOTE-001 was the first trial to demonstrate the activity of the PD-1 inhibitor pembrolizumab in patients with treatment-naïve or previously treated advanced NSCLC. Notably, in this multicohort phase IB study, pembrolizumab showed greater activity with increasing PD-L1 tumor proportion score (TPS). Between May 2012 and July 2014, 550 patients with advanced NSCLC had been enrolled across 4 non-randomized and 2 randomized cohorts.
Novel first-line options and other insights in EGFR-mutant lung cancer
Although treatment with EGFR TKIs is generally efficient in patients with EGFR-mutant lung cancer, resistance inevitably develops within 8 to 12 months of the initiation of therapy, leading to treatment failure. Therefore, there is an unmet need for options that extend the activity of EGFR-targeted therapies. Dual blockade of the VEGF and EGFR signaling pathways represents a potential approach in this respect.
Early-stage NSCLC: promising (neo)adjuvant approaches
Effective treatment options are called for in patients with resectable non-small-cell lung cancer (NSCLC), as more than half of those with stage I to III disease experience relapses [1]. Chen et al. demonstrated in their animal model that tumor PD-L1 upregulation is critical for the spread and survival of metastases [2]. Based on these considerations, several clinical trials are investigating the potential benefits of immunotherapies in the neoadjuvant setting.