Metastatic NSCLC: new drugs and updates in well-known agents
Squamous-cell carcinoma: nedaplatin
Tumours with squamous histology account for 20 % to 30 % of cases of non–small-cell lung cancer (NSCLC).
Despite this substantial proportion, only limited progress has been made in the treatment of advanced squamous-cell carcinoma (SCC) compared to non-squamous NSCLC, and thus SCC of the lung is a disease with a high unmet medical need.
In the field of chemotherapy, cisplatin plus docetaxel is standard-of-care in patients with advanced SCC of the lung. Nedaplatin is a second-generation platinum compound with reduced toxicity. Based on the WJOG5208L trial, it can be considered as a new standard treatment for advanced or relapsed SCC [1]. This study compared docetaxel 60 mg/m2 plus nedaplatin 100 mg/m2 every 3 weeks for 4 to 6 cycles with the standard regimen of docetaxel and cisplatin. A total of 349 chemo-naïve patients with stage IIIb/IV or recurrent SCC who were not amenable to curative-intent radiation therapy participated in the trial.
For the primary endpoint of overall survival (OS) in the WJOG5208L trial, the new combination regimen showed significant benefit over the control arm (13.6 vs. 11.4 months; hazard ratio [HR] 0.81; p = 0.037). However, progression-free survival (PFS) did not differ between the two arms, as also seen for objective response rate (ORR) and disease control rate (DCR). Grade ≥ 3 adverse events (AEs) occurred to a similar extent in both treatment arms, whereas AEs leading to discontinuation of the study drug were more frequent in the control arm (15.3 % vs. 23.3 %). The experimental arm showed advantages regarding incidence of nausea/vomiting and electrolyte imbalance, whereas myelosuppression was more frequent and more severe than in the patients in the control arm. This increase did not translate into higher rates of febrile neutropenia or bleeding, however.
Afatinib-mediated survival benefit
Activating epidermal growth factor receptor (EGFR) mutations including the exon 21 L858R mutation and exon 19 deletions are key drivers of NSCLC in 10 % to 15 % of patients of European descent, and in 30 % to 35 % of those of Asian descent. EGFR tyrosine kinase inhibitors (TKIs) are recommended as first-line therapy in EGFR-mutation-positive advanced NSCLC. Among these agents, afatinib appears to be the TKI of choice in the second-line treatment of patients with SCC of the lung. This insight is derived from the LUX-Lung 8 global phase III trial, the largest phase III trial ever conducted in the second-line treatment setting of SCC of the lung. Here, the reversible EGFR TKI erlotinib was compared with afatinib. In contrast to erlotinib, afatinib is an irreversible TKI, and its effects extend to ErbB1 (EGFR), HER2 and HER4. The study authors hypothesised that afatinib would confer additional benefits over erlotinib due to its broader signal-transduction inhibition. Thus, for LUX-Lung 8, a total of 795 patients with SCC of the lung (stage IIIB/IV) who had progressed after at least 4 cycles of a first-line platinum doublet were randomised to either afatinib 40 mg daily (QD) or erlotinib 150 mg QD.
The primary endpoint was defined as PFS by independent review. This was met according to the primary PFS analysis that was presented at the ESMO Congress 2014 [2]. At the ASCO Congress 2015, the median OS (key secondary endpoint) with afatinib and erlotinib was shown to be 7.9 months and 6.8 months, respectively, which translated into a 19 % reduction in mortality risk (HR, 0.81; p = 0.0077; Figure 1) [3]. The survival curves separated early on, which reflects a consistent advantage of afatinib. Landmark analyses at 12 and 18 months demonstrated higher percentages of patients alive in the afatinib arm (36.4 % vs. 28.2 %, 22.0 % vs. 14.4 %, respectively). All subgroup analyses favoured afatinib over erlotinib, independent of age, gender, ethnicity, smoking history, histology, and best response to first-line chemotherapy.

Figure 1: Significant OS benefit with afatinib over erlotinib in the LUX-Lung 8 trial for pre-treated patients with squamous-cell histology
LUX-Lung 8: patient-reported outcomes and adverse events
The updated PFS analysis of LUX-Lung 8 was in keeping with the data obtained at the first analysis, with a 19 % reduction in the risk of progression (median PFS, 2.6 vs. 1.9 months; HR, 0.81; p = 0.0103). The ORR favoured afatinib numerically (5.5 % vs. 2.8 %; p = 0.055). However, the benefit gained by afatinib therapy is basically due to disease stabilisation. The DCR was 50.5 % vs. 39.5 % for afatinib and erlotinib, respectively, and this difference was significant (p = 0.002). Patient-reported outcomes were acquired by means of standard European Organisation for Research and Treatment of Cancer (EORTC) questionnaires that focussed on dyspnoea, cough, and pain, with global health status also evaluated [4]. Symptom relief and quality of life improvement were more pronounced with afatinib than erlotinib. This also applied to the time to deterioration.
Overall, AEs were balanced between both arms. The AEs that led to dose reduction were more frequent with afatinib as compared to erlotinib, but the proportions of AEs prompting discontinuation were similar. The most common drug-related AEs matched the overall safety profiles that have been described for these two treatments. Diarrhoea and stomatitis occurred predominantly with afatinib, whereas grade 3 rash was observed more frequently with erlotinib.
A tumour genomic analysis is ongoing. So far, 238 patients have been analysed. The results show that EGFR aberrations are infrequent and are balanced between the two arms.
No correlations of EGFR aberrations with PFS or OS were found. Therefore, the EGFR mutation status cannot explain the added benefit of afatinib over erlotinib.
Mutant-selective EGFR inhibition
Patients with activating EGFR mutations typically experience good initial responses to therapy with first-generation EGFR TKIs (e.g., erlotinib, gefitinib) and with the second-generation TKI afatinib. However, after 9 months to 14 months of treatment, disease progression invariably ensues. In 50 % to 60 % of patients, this is driven by a secondary T790M ‘gatekeeper’ mutation in exon 20. Furthermore, approximately 2 % to 3 % of patients with EGFR-mutant NSCLC have this T790M mutation at baseline. For this group of patients, no approved therapies exist, and they show very poor outcomes with the currently available TKIs.
Third-generation EGFR TKIs that address this need have been developed. AZD9291 is an oral irreversible EGFR TKI that shows selectivity for sensitising and for T790M resistance mutations. The AURA phase I dose-escalation/expansion study demonstrated encouraging clinical activity of AZD9291 as first-line treatment in 160 patients with EGFR-mutation-positive, locally advanced or metastatic NSCLC [5]. With AZD9291 80 mg QD and 160 mg QD, the ORRs were 63 % and 83 %, respectively. Although these data were still too immature to estimate the median PFS, the PFS analysis at 12 months yielded a high rate of 72 %. The tolerability profile also proved manageable. AZD9291 80 mg is currently being tested in the phase III FLAURA study, in comparison with gefinitib 250 mg QD and erlotinib 150 mg QD.
Compelling activity of rociletinib
Rociletinib is another orally administered third-generation EGFR TKI, which irreversibly inhibits activating EGFR mutations as well as the T790M mutation, while wild-type EGFR is spared. The phase I/II TIGER-X trial assessed rociletinib in patients with advanced or recurrent NSCLC who had received prior treatments with EGFR-directed therapy and showed documented activating EGFR mutations [6]. The phase II expansion cohort contained second-line patients after progression on EGFR-directed therapy, as well as patients beyond second line, who had progressed on two or more TKIs or chemotherapy. Their biopsies had to be positive for the T790M mutation at study entry. Treatment was administered at four different doses: 500 mg twice daily (BID), 625 mg BID, 750 mg BID, and 1,000 mg BID.
In the 243 patients included with centrally confirmed T790M mutation, the ORR and DCR were 53 % and 85 %, respectively (Table). The response rates did not vary significantly by dose. PFS estimates are immature, as the study is still ongoing. At the time of the analysis, median PFS was 8.0 months in patients with centrally confirmed T790M mutation. In the group without central nervous system (CNS) disease at baseline, it was 10.3 months. Rociletinib was also shown to have activity in T790M-negative patients, with an ORR of 37 %. Furthermore, TIGER-X demonstrated that T790M plasma testing using the quantitative and sensitive BEAMing Test is a viable alternative to tissue testing. The ORRs obtained with both methods were similar.
Hyperglycaemia with rociletinib: frequent, but manageable
Rociletinib was generally well tolerated, with the primary side effect being hyperglycaemia, which was often accompanied by diarrhoea, nausea and decreased appetite. The 500 mg dose level showed an improved safety profile compared to the higher dose levels. In this group, the rate of grade 3/4 hyperglycaemia was lowest at 17 %. Also, no cases of interstitial lung disease have been observed in the 500 mg dose group, although seven cases occurred in TIGER-X overall. Treatment-related AEs that led to drug discontinuation were less frequent with 500 mg BID than in the total cohort (2.5 % vs. 4 %).
Hyperglycaemia is caused by iatrogenic insulin resistance due to a rociletinib metabolite. It can be managed through a monitoring and treatment algorithm that uses oral agents. These are very successful in treating the hyperglycaemia as well as in relieving the associated gastrointestinal symptoms.
On the grounds of the assumption that early targeting of the T790M mutation along with initial activating mutations is a rational approach to impeding disease progression, the randomised, open-label, phase II/III study TIGER-1 is currently investigating rociletinib in the first-line setting as compared to erlotinib, in patients with EGFR-mutant NSCLC [7]. The phase III, open-label, randomised TIGER-3 trial is comparing rociletinib with single-agent cytotoxic chemotherapy in patients with EGFR-mutant NSCLC who have shown progression on at least one previous EGFR TKI therapy and platinum-based doublet chemotherapy [8]. The rationale for the TIGER-3 trial is that patients who fail on chemotherapy and first-generation EGFR TKIs have limited treatment options.
EGFR wild-type NSCLC
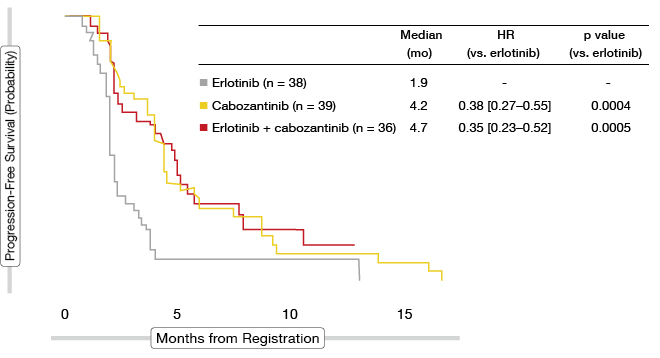
As erlotinib has only modest activity in unmutated EGFR NSCLC, administration of the oral small-molecule multikinase inhibitor cabozantinib alone or in combination with erlotinib might improve efficacy in these patients. The randomised phase II E1512 trial tested erlotinib 150 mg QD, cabozantinib 60 mg QD, and erlotinib 150 mg QD plus cabozatinib 40 mg QD, as second-line or third-line therapy in 125 patients with EGFR-mutation-negative, metastatic non-squamous NSCLC [9]. The median PFS in each cabozantinib arm in comparison to the erlotinib-only control arm was defined as the primary endpoint.
Indeed, the PFS results were improved with cabozantinib monotherapy as well as with the erlotinib plus cabozantinib combination, compared to erlotinib monotherapy (median PFS, 4.2 vs. 4.7 vs. 1.9 months, respectively; Figure 2). The differences between the two experimental arms and the erlotinib arm were statistically significant (p = 0.0004, 0.0005, respectively) and these translated into risk reductions of > 60 %. Similarly, for OS, the cabozantinib-treated patients fared significantly better. This was particularly true for the combination group, whereby the median OS was 4.1 months for the control arm, but as high as 13.3 months for the erlotinib plus cabozantinib arm (p = 0.004) and 9.2 months for the cabozantinib-only arm (p = 0.03). Thus, compared to erlotinib, the mortality risk was reduced by 56 % and 41 %, respectively. However, the follow-up is currently short on the combination arm, so that the results might change with further analysis. Responses were noted relatively infrequently across the three arms, ranging from 3 % to 14 %. However, disease stabilisation was much more common with the combination and with cabozantinib alone than with erlotinib monotherapy (42 % and 45 % vs. 17 %, respectively).
Tissue was collected in all patients with the intention of MET immunohistochemistry (IHC) testing. The comparison of the treatment effects on MET-positive tumours was defined as a secondary outcome. According to this analysis, the total MET IHC status did not appear to be predictive of PFS for cabozantinib treatment. A follow-up study is currently being planned.
Efficacy of cabozantinib in RET rearrangement
Cabozantinib also appears to be active in tumours that show RET rearrangements, which are characterised by fusions of intact tyrosine kinase domains to upstream gene partners. These aberrations are found in 1 % to 2 % of NSCLCs, and they are drivers of cell growth in vitro and in vivo. Clinical features of patients with RET rearrangements comprise young age and never-smoking status, or former light smoking. Adenocarcinoma is the most common histology.
A phase II, open-label trial evaluated cabozantinib 60 mg daily in patients with stage IV NSCLC with RET rearrangements [10]. In stage 1 of the trial, 16 patients were included, with one response required to move on to stage 2, which is currently accruing nine additional patients. Here, responses in five cases are required to meet the primary endpoint of overall response.
At the completion of stage 1, the ORR was 38 %, and another 56 % of patients experienced disease stabilisation. The median duration of response was 8 months, the median PFS was 7 months, and the median OS was 10 months. The most common AEs included transaminase elevations, diarrhoea, fatigue, mucositis, skin and hair hypopigmentation, palmar-plantar erythrodysaesthesia, and decreased platelet counts. While the overall rates of AEs were high, grade 3 events were rare. The majority of patients required at least one dose reduction during the course of therapy; however, clinical benefit was maintained in spite of these dose reductions.
BRAF-mutated tumours: dabrafenib and trametinib
Another genetic aberration to be found in NSCLC is BRAF mutations. These mutations are present in approximately 2 % of patients. BRAFV600E-mutated tumours typically show histologic features that are suggestive of aggressive tumour biology, and the patients affected have less-favourable outcomes when treated with platinum-based chemotherapy.
The small molecules dabrafenib and trametinib both inhibit the MAP kinase (MAPK) pathway by targeting BRAF V600 kinase and MEK signalling, respectively, thus antagonising cell proliferation, growth and survival in different tumour types. A multicentre, open-label, phase II study (BRF113928) tested dabrafenib as monotherapy (n = 60) and in combination with trametinib (n = 40) in patients with BRAFV600E-mutated, stage IV NSCLC who had received at least one previous platinum-based chemotherapy [11].
At the time of the interim analysis of BRF113928, 82 % of the patients were still on study treatment, and dabrafenib plus trametinib showed clinically meaningful anti-tumour activity. In the combination group, 63 % and 25 % of patients achieved partial responses and stable disease, respectively, giving a DCR of 88 %. With monotherapy, the ORR and DCR were 32 % and 56 %, respectively. The median duration of response had not been reached in the second-line setting and beyond. The safety profile proved manageable and similar to previous studies in melanoma. AEs leading to dose reduction occurred in 27 % of patients, and dose interruptions were necessary in 52 %. A third cohort that is investigating dabrafenib plus trametinib in previously untreated BRAF-mutated, stage IV NSCLC is actively recruiting at present.
ALK rearrangements as a therapeutic target
The ALK-specific TKI crizotinib is an established option in pre-treated patients with ALK-rearranged NSCLC. However, acquired resistance mutations in the ALK gene are a common cause of progression. Also, in spite of potential CNS disease control, approximately half of the patients develop brain metastases during crizotinib treatment.
The highly selective oral ALK inhibitor alectinib is active against most clinically relevant acquired ALK-resistance mutations. In the phase II NP28673 trial, patients with ALK-positive NSCLC who did not respond to or had progressed on prior crizotinib treatment received alectinib 600 mg BID [12]. Overall, 138 people participated in this study, and the response-evaluable cohort comprised 122 patients. The co-primary endpoint was ORR by Independent Review Committee in two populations: in all of the patients, and in those who had received prior chemotherapy.
The analysis yielded a robust response rate of 50 %. For the chemotherapy-naïve and chemotherapy-treated patients, the rates were 69.2 % and 44.8 %, respectively. Disease control was obtained in 78.7 % in the total population; also, the duration of response was remarkably long, at 11.2 months. Median PFS was 8.9 months. Alectinib showed considerable activity in patients with measurable brain metastases, irrespective of prior irradiation (Figure 3). In this cohort, the analysis revealed an excellent DCR of 85.7 %. Objective CNS response was observed in 57.1 %, and complete remission occurred in 20.0 %. CNS response lasted for 10.3 months. Alectinib also demonstrated a favourable safety and tolerability profile. Most common AEs included constipation, fatigue, peripheral oedema, and myalgia. There were only a few reported grade 3/4 AEs. The ALEX phase III study is currently investigating first-line alectinib 600 mg BID compared to crizotinib 250 mg BID in patients with stage IIIb/IV or recurrent NSCLC.
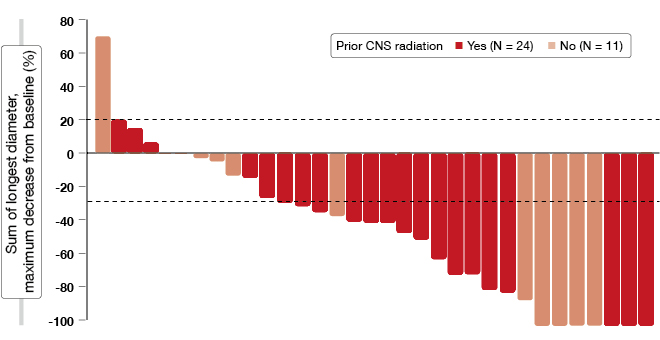
Figure 3: Marked activity of alectinib in ALK-positive NSCLC patients with measurable CNS disease
Omission of whole-brain radiotherapy
After radical treatment of primary NSCLC, the brain remains a frequent and early site of distant relapse, with CNS metastases affecting up to 40 % of patients. Patients with NSCLC and brain metastases fare poorly, even if irradiated. In spite of a lack of randomised, controlled data, whole-brain radiotherapy (WBRT) plus steroid therapy is the present standard of care.
The randomised, controlled, non-inferiority QUARTZ trial investigated the omission of WBRT in patients with NSCLC and brain metastases who were unsuitable for resection or stereotactic radiosurgery [13]. While the control arm received optimal supportive care (OSC), including dexamethasone and WBRT 20 Gy/5f, patients in the investigational arm were treated with OSC and dexamethasone only. The primary outcome was quality-adjusted life years (QALYS). Each arm contained 269 patients from the UK and Australia, and > 70 % of the patients in both arms suffered from moderate or severe symptoms, with the majority requiring steroid treatment.
The analysis showed that the OS did not differ between the two arms (9.3 vs. 8.1 weeks in the OSC plus WBRT group and the OSC alone group, respectively; HR, 1.05; p = 0.52). For the primary outcome measure, there was a difference in QALYS of 1.9 days that favoured the WBRT arm, which stayed below the non-inferiority boundary. According to the conclusion of the authors, this suggests that WBRT provides no additional clinically significant benefit in this group of patients. Also, WBRT did not appear to be a steroid-sparing treatment modality.
REFERENCES
- Shukuya T et al., Randomized phase III study of nedaplatin (N) plus docetaxel (D) versus cisplatin (C) plus D for advanced or relapsed squamous cell carcinoma of the lung (SqLC): WJOG5208L. J Clin Oncol 33, 2015 (suppl; abstr 8004)
- Goss G et al., A randomized, open-label, phase III trial of afatinib (A) vs erlotinib (E) as second-line treatment of patients (pts) with advanced squamous cell carcinoma (SCC) of the lung following first line therapy. Ann Oncol 2014; 25(Suppl 4); iv426-iv470 (abstr 1222O)
- Soria JC et al., Afatinib (A) vs erlotinib (E) as second-line therapy of patients (pts) with advanced squamous cell carcinoma (SCC) of the lung following platinum-based chemotherapy: Overall survival (OS) analysis from the global phase III trial LUX-Lung 8 (LL8). J Clin Oncol 33, 2015 (suppl; abstr 8002)
- Gadgeel SM et al., Afatinib (A) vs erlotinib (E) as second-line treatment of patients (pts) with advanced squamous cell carcinoma (SCC) of the lung following first-line platinum-based chemotherapy: Patient-reported outcome (PRO) data from the LUX-Lung 8 Phase III global trial. J Clin Oncol 33, 2015 (suppl; abstr 8100)
- Ramalingam SS et al., AZD9291, a mutant-selective EGFR inhibitor, as first-line treatment for EGFR mutation-positive advanced non-small cell lung cancer (NSCLC): Results from a phase 1 expansion cohort. J Clin Oncol 33, 2015 (suppl; abstr 8000)
- Sequist LV et al., Efficacy of rociletinib (CO-1686) in plasma-genotyped T790M-positive non-small cell lung cancer (NSCLC) patients (pts). J Clin Oncol 33, 2015 (suppl; abstr 8001)
- Ross Camidge D et al., TIGER 1: A randomized, open-label, phase 2/3 study of rociletinib (CO-1686) or erlotinib as first-line treatment for EGFR-mutant non-small cell lung cancer (NSCLC). J Clin Oncol 33, 2015 (suppl; abstr TPS8108)
- Yang J C-H et al., TIGER-3: A phase 3, open-label, randomized study of rociletinib vs cytotoxic chemotherapy in patients (pts) with mutant EGFR non-small cell lung cancer (NSCLC) progressing on prior EGFR TKI therapy and doublet chemotherapy. J Clin Oncol 33, 2015 (suppl; abstr TPS8109)
- Neal JW et al., Cabozantinib (C), erlotinib (E) or the combination (E+C) as second- or third-line therapy in patients with EGFR wild-type (wt) non-small cell lung cancer (NSCLC): A randomized phase 2 trial of the ECOG-ACRIN Cancer Research Group (E1512). J Clin Oncol 33, 2015 (suppl; abstr 8003)
- Drilon AE et al., Phase II study of cabozantinib for patients with advanced RET-rearranged lung cancers. J Clin Oncol 33, 2015 (suppl; abstr 8007)
- Planchard D et al., Interim results of a phase II study of the BRAF inhibitor (BRAFi) dabrafenib (D) in combination with the MEK inhibitor trametinib (T) in patients (pts) with BRAF V600E mutated (mut) metastatic non-small cell lung cancer (NSCLC). J Clin Oncol 33, 2015 (suppl; abstr 8006)
- Ou S-H I et al., Efficacy and safety of the ALK inhibitor alectinib in ALK+ non-small-cell lung cancer (NSCLC) patients who have failed prior crizotinib: an open-label, single-arm, global phase 2 study (NP28673). J Clin Oncol 33, 2015 (suppl; abstr 8008)
- Mulvenna PM et al., Whole brain radiotherapy for brain metastases from non-small lung cancer: Quality of life (QoL) and overall survival (OS) results from the UK Medical Research Council QUARTZ randomised clinical trial (ISRCTN 3826061). J Clin Oncol 33, 2015 (suppl; abstr 8005)
More posts
Metastatic NSCLC: new drugs and updates in well-known agents
Tumours with squamous histology account for 20 % to 30 % of cases of non–small-cell lung cancer (NSCLC). Despite this substantial proportion, only limited progress has been made in the treatment of advanced squamous-cell carcinoma (SCC) compared to non-squamous NSCLC, and thus SCC of the lung is a disease with a high unmet medical need.
Preface – ASCO 2015
As for many other oncological diseases, the management of lung cancer has undergone major changes in the last few years with the rise of targeted therapies, and more lately, of immunotherapy. These advances are reflected in the results of experimental research and clinical trials that were presented at the Annual Meeting of the American Society of Clinical Oncology that took place in Chicago, from 29th May to 2nd June, 2015.