Risks and chances in patients with oligometastatic disease
Against the background of improved systemic therapies, there are rising expectations with regard to the potential cure of NSCLC patients who have a limited number of haematogeneous metastases. “Most studies define oligometastasis as one to three, or one to five lesions,” explained Suresh Senan, MRCP, FRCR, PhD, VU University Medical Centre, Amsterdam, The Netherlands [1]. Depending on the clinical scenario, there are synchronous (detection at the time of diagnosis of the primary tumour) and metachronous (development after treatment of the primary tumour) oligometastases. As Dr. Senan pointed out, the interval that allows for differentiation between these two is not standardised, but a time span of 6–12 months is commonly used.
The term of oligorecurrence describes oligometastasis in the setting of a controlled primary tumour. ‘Oligoprogression’, on the other hand, refers to progression of a limited number of known metastatic lesions, while all other metastases are controlled with systemic therapy.
Identification of prognostic factors
Ablative therapies include surgical resection, stereotactic radiotherapy, and radiofrequency ablation. However, there is a general lack of evidence with respect to these treatments, and data can be unreliable due to several types of bias, including selection bias or immortal time bias. “The only high-level evidence according to which aggressive treatment of metastases improves survival has been obtained in patients with brain metastases”, reported Dr. Senan. A trial published in 1990 showed that addition of surgical resection to whole-brain radiotherapy (WBRT) in patients with a single brain lesion improved median OS from 15 to 40 weeks [2]. According to another study, in patients with up to three CNS metastases, radiosurgery in addition to WBRT provided an OS benefit (6.5 months vs. 4.9 months with WBRT alone) [3].
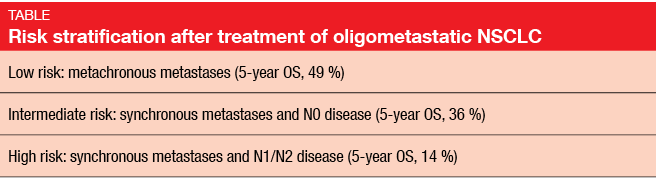
A meta-analysis of 757 NSCLC patients with one to five synchronous or metachronous metastases investigated factors for good prognosis after treatment [4]. “These were generally younger patients with a good performance status,” said Dr. Senan. Importantly, after exclusion of metastatic disease, two thirds had early-stage intra-thoracic disease (IA-IIB rather than stage III). Thus, they were hardly representative of the average NSCLC patient population. Median OS was favourable at 26 months, and the 5-year OS rate was 30 %. The researchers identified the following predictors for improved OS: metachronous versus synchronous metastases (p < 0.001), N stage (p = 0.002), and adenocarcinoma histology (p = 0.036). Three risk groups were defined through recursive partitioning analysis (Table).
Irradiation techniques
Stereotactic body radiotherapy (SBRT) is a technique for delivering high-dose external beam radiotherapy to an extra-cranial target with a high degree of accuracy. The largest series of patients treated with SBRT for oligometastatic disease included 321 cancer patients from Denmark [5]. Favourable prognostic factors were performance status of 0–1, solitary metastasis, diameter of metastatic lesions < 30 mm, metachronous metastases, and pre-SBRT chemotherapy. OS after SBRT declined considerably when four or more unfavourable factors were present (Figure).
Stereotactic radiosurgery (SRS) is an accepted treatment modality for patients with one to four brain lesions that measure 4 cm or less in diameter [6]. SRS alone or in combination with surgical resection or WBRT can lead to good local control in patients with brain metastases. The role of WBRT is currently under debate. A pooled analysis from three phase III trials in a total of 264 patients showed that in patients aged 50 years or younger, WBRT can be omitted without any detrimental effects [7]. SRS as a stand-alone therapy was sufficient in this group. Similarly, there was an age effect for out-of-field brain metastases (distant brain failure): younger patients experienced no increased risk of out-of-field cerebral relapse with SRS alone, while the addition of WBRT reduced the risk for those over 50 years of age. “Part of the debate relates to whether it is necessary to irradiate an elderly brain,” said Dr. Senan. “Many of us have these patients undergo MRI follow-up every three months and treat subsequent metastases when they appear.”
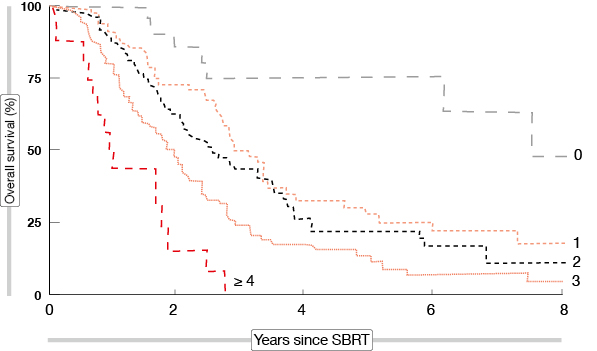
Figure: Survival after SBRT according to the number of unfavourable prognostic factors
Patients with EGFR or ALK aberrations
Given the wealth of new treatment options, a question that needs to be answered is whether ablative radiotherapy complements targeted agents and immunotherapies. In TKI-treated patients, irradiation is obviously not urgently required after the detection of asymptomatic metastatic brain lesions. “We can wait for systemic therapy to start working”, Dr. Senan explained. Once progression sets in, there is a reasonable chance of achieving local control. Alectinib-treated patients with ALK-rearranged, crizotinib-refractory NSCLC and baseline CNS metastases (measurable or non-measurable) without prior radiation showed a complete CNS response rate of 43 % in a global phase II trial [8]. Those with measurable baseline lesions attained a CNS ORR of 57 %. According to the ESMO guidelines from 2014, oligometastatic progression during targeted treatment can be ablated with local treatment (such as surgery or radiotherapy), while TKI therapy is continued or resumed [6]. Before proceeding with local therapy, a full evaluation of the extent of the disease, including CNS imaging, is recommended.
“At present, we prefer to go for systemic treatment in patients without a high symptom burden,” Dr. Senan reported. “If they progress, on-demand stereotactic radiotherapy is used.” Local treatment that is limited to specific lesions, which are suspected to cause the patient’s symptoms, are an option while systemic therapy continues.
Radiation plus immunotherapy: boosting the local immune system
Yet another challenge arises in the context of immunotherapy, because radiotherapy has been shown to have both immunomodulatory and immunosuppressive effects. Irradiation induces tumour cell apoptosis, release of tumour antigens, and expression of immunogenic cell death receptors, like calreticulin and HMGB-1, as well as up-regulation of immunogenic cell-surface markers, such as MHC-1 [9]. Homing of immune cells and antigen presentation are improved. On the other hand, PD-L1 expression also increases, and Langerhans cells in the skin migrate to lymph sites, which results in up-regulation of regulatory T cells [10].
One of the peculiarities of radiotherapy that has attracted attention is the relatively uncommon phenomenon of abscopal effects. This term refers to regression of non-irradiated metastatic lesions that are distant from an irradiated tumour site. These responses are believed to be immune mediated [11]. “The idea is that radiotherapy combined with immunotherapy might increase the abscopal effect,” Dr. Senan pointed out [12]. “The treatment could thus be given a kick-start, and prediction of response might be improved.” Issues such as optimal sequencing and radiation dosing remain unclear, however.
Current dilemmas
To date, safety data for sequencing or combining irradiation with new agents are lacking. This is all the more relevant as drugs are being approved at a rapid pace. “We are now much more careful regarding the choice of radiation techniques,” Dr. Senan emphasised. When complications occur, such as bowel perforation in a TKI-treated patient, it is difficult to identify the actual cause. Moreover, it happens that recommendations are sometimes contradictory within the multidisciplinary team. “The pulmonologist might instruct the patients to continue their systemic treatment, while the radiation oncologist may ask them to stop it until the radiotherapy is completed.”
Overall, as high-quality evidence still needs to be generated, caution is required regarding the multimodal approach. “Potential benefits must be balanced against the risks of unexpected morbidity and mortality,” Dr. Senan summarised.
Source: Educational Session: Optimal therapy for earlier stages of NSCLC, 21st December, 2015
REFERENCES
- Palma DA et al., The oligometastatic state – separating truth from wishful thinking. Nat Rev Clin Oncol 2014; 11(9): 549-557
- Patchell RA et al., A randomized trial of surgery in the treatment of single metastases to the brain. New Engl J Med 1990; 322(8): 494-500
- Andrews DW et al., Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet 2004; 363(9422): 1665-1672
- Ashworth AB et al., An individual patient data meta-analysis of outcomes and prognostic factors after treatment of oligometastatic non-small-cell lung cancer. Clin Lung Cancer 2014; 15(5): 346-355
- Fode MM & Høyer M, Survival and prognostic factors in 321 patients treated with stereotactic body radiotherapy for oligo-metastases. Radiother Oncol 2015; 114(2): 155-160
- Besse B et al., 2nd ESMO Consensus Conference on Lung Cancer: non–small-cell lung cancer first-line/ second and further lines of treatment in advanced disease. Ann Oncol 2014; 25(8): 1475-1484
- Sahgal A et al., Phase 3 trials of stereotactic radiosurgery with or without whole-brain radiation therapy for one to four brain metastases: individual patient data meta-analysis. Int J Radiat Oncol Biol Phys 2015; 91(4): 710-717
- Ou S-H et al., Alectinib in crizotinib-refractory ALK-rearranged non–small-cell lung cancer: a phase II global study. J Clin Oncol 2015; Nov 23. pii: JCO639443. [Epub ahead of print]
- Daly ME et al., Clinical trials integrating immunotherapy and radiation for non–small-cell lung cancer. J Thorac Oncol 2015; 10(12): 1685-1693
- Zitvogel L & Kroemer G, Subversion of anticancer immunosurveillance by radiotherapy. Nat Immunol 2015; 16(10): 1005-1007
- Grimaldi AM et al., Abscopal effects of radiotherapy on advanced melanoma patients who progressed after ipilimumab immunotherapy. Oncoimmunology 2014; 3: e28780
- Postow MA et al., Immunologic correlates of the abscopal effect in a patient with melanoma. N Engl J Med 2012; 366(10): 925-931
More posts
Preface – ESMO Asia 2015
My career in lung cancer care started at a time when nihilism prevailed and the standard approach in advanced disease consisted of best supportive measures. No treatments were available in which the benefits outweighed the toxicity. The arrival of chemotherapy eventually rendered improvements in survival possible; in addition, this strategy allowed for symptom relief and increases in quality of life.