Advancing treatment in patients with mantle cell lymphoma
Update on acalabrutinib monotherapy
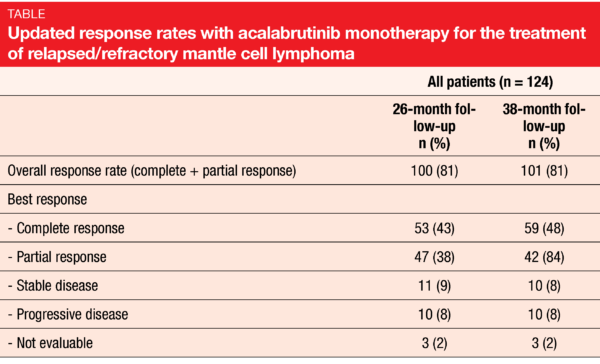
High relapse rates after standard-of-care regimens in the frontline setting are typical of mantle cell lymphoma (MCL), which is an aggressive, rare, B-cell Non-Hodgkin lymphoma [1-4]. The second-generation, highly selective BTK inhibitor acalabrutinib has been approved in the US for the treatment of patients with MCL after ≥ 1 prior therapy based on the single-arm, open-label, multicenter, phase II ACE-LY-004 study [5]. At ASH 2020, Wang et al. reported updated efficacy and safety results from this trial after an additional year of follow-up [6]. A total of 124 patients with r/r MCL were enrolled. At a median follow-up of 38.1 months, 55 (44 %) remained on study, with 24 (19 %) still receiving acalabrutinib.
According to the updated findings, treatment efficacy was largely maintained. The ORR was 81 %, as it had been after the 26-month follow-up at the time of the primary analysis (Table) [5]. Complete responses had increased from 43 % to 48 %. Median duration of response amounted to 28.6 months. At 36 months, 41.9 % of patients responded, and 37.2 % were progression-free. Median PFS was 22.0 months. Median OS had not been reached yet, and the 36-month OS rate was 60.5 %. Six of 30 patients (20 %) with available samples maintained complete remission and undetectable minimal residual disease at the last assessment.
Moreover, the extended follow-up conveyed no new safety concerns. The AE profile was basically unchanged, with infections and bleeding events occurring as the most common toxicities. More than half of patients with any bleeding event were receiving anticoagulant medication. AEs led to dose delays in 50 patients (40 %) and dose modifications in 2 (2 %). There were 57 deaths (46 %), most commonly due to disease progression (n = 38; 31 %). Overall, these data confirmed the safety and efficacy of acalabrutinib in patients with r/r MCL.
Frontline ibrutinib + rituximab in the elderly
Many elderly patients suffering from MCL are transplant-ineligible and not suitable for intensive chemoimmunotherapy due to comorbidities. The combined use of ibrutinib and rituximab was tested in a single-center, phase II study containing 50 previously untreated MCL patients aged ≥ 65 years with ECOG performance status ≤ 2 and normal organ function [7]. Their median age was 71 years. Bone marrow involvement was present in 94 %. Twenty-five percent had a Ki-67 index ≥ 30-50 %.
Overall, 90 % of patients responded to the treatment, with 62 % and 28 % achieving complete and partial remissions, respectively. MRD negativity at the time of the best response was 87 %. Median PFS and OS had not been reached yet at a median follow-up of 43 months. Out of 4 patients who progressed, 3 showed transformation to the blastoid/pleomorphic variant. Two had Ki-67 ≥ 30 %, one was TP53-mutated, and another had FAT1 and SF3B1 mutations. Five patients died off study; in 3 cases, this was due to progression, and in 2, the etiology was unknown. Among AEs, fatigue, diarrhea and myalgia occurred most frequently. Seventeen patients (34 %) developed atrial fibrillation. Median time to onset from the start of treatment was 9.4 months.
The authors noted that ibrutinib plus rituximab is a highly effective, easily administered, chemotherapy-free option for transplant-ineligible elderly patients with non-blastoid (Ki-67 < 50 %) MCL. The increased incidence of arrhythmia observed in the study was likely due to the high number of cardiovascular risk factors in this population. This suggested that baseline cardiac evaluation and cardiovascular risk factor modification should be performed in the context of treatment with ibrutinib and rituximab. The long-term follow-up will reveal the impact of the combined treatment on safety and relapse patterns.
Orelabrutinib gives rise to high CR rates
A multicenter, open-label, phase II study tested the efficacy and safety of the novel, highly selective, irreversible BTK inhibitor orelabrutinib as monotherapy in Chinese patients with r/r MCL [8]. The safety population comprised 106 patients, and 99 made up the efficacy population. Orelabrutinib was administered at doses of 100 mg twice daily (n = 20) and 150 mg/d (n = 86).
The treatment gave rise to marked responses and durable remissions. At 16.4 months, the ORR was 87.9 %, with a CR rate of 34.3 % by CT-based imaging. These results represented slight increases compared to the ORR and CR of 85.9 % and 30.3 %, respectively, observed at 10.5 months. Complete responses according to PET-CT had even been achieved in 42.9 %. The disease control rate added up to 93.9 %. At 12 months, 70.8 % of patients were progression-free, and 88.7 % were alive. Median PFS and duration of response had not been reached yet at the time of the analysis.
Orelabrutinib showed a favorable safety profile. Treatment-related AEs leading to dose reductions and study drug discontinuation occurred in 6.6 % and 2.8 %, respectively. Thrombocytopenia, neutropenia and upper respiratory tract infections were most commonly reported. Among AEs of special interest, hemorrhage was most common but was restricted to grade 1 and 2. Moreover, no grade ≥ 3 atrial fibrillation/flutter or grade ≥ 3 diarrhea occurred. Grade ≥ 3 infections were observed in 12.3 %. As the authors noted in their conclusion, the pronounced efficacy and improved safety of orelabrutinib resulting from its high target selectivity, combined with the convenience of daily dosing, mark this agent as a preferable option for the treatment of patients with B-cell malignancies.
Parsaclisib in BTK-inhibitor–pretreated patients…
The CITADEL-205 study evaluated the highly selective, next-generation PI3Kδ inhibitor parsaclisib in the setting of r/r MCL. Cohort 1 of the study contained patients who had previously received BTK inhibition, while those in Cohort 2 were BTK-inhibitor–naïve. In both groups, 1–3 prior lines of systemic therapy had been administered. Parsaclisib 20 mg for 8 weeks was followed by either 20 mg once weekly (weekly group) or 2.5 mg once daily continuously (daily group). During the study, the daily group dose was selected as the preferred dosing regimen, and patients in the weekly group were allowed to switch to the daily group. The findings for the overall and daily groups were reported at ASH 2020 for Cohorts 1 and 2 separately.
Zinzani et al. presented the results for the BTK-inhibitor–pretreated Cohort 1 which consisted of a total of 53 patients, with 41 treated in the daily group [9]. The ORRs according to independent review were 25 % and 29 % (Figure) for the overall and daily groups, respectively. CRs resulted in 2 % each, and PRs and 23 % and 27 %, respectively. Forty-seven percent of all treated patients and 51 % of those in the daily group had regression of target lesions. Median duration of response amounted to 3.7 months in both groups; likewise, median PFS was 3.7 across all patients. Median OS was 11.2 in both the total cohort and the daily group. Estimated survival rates at 18 months were 32 % and 37 %, respectively.
… and those without BTK inhibitor pretreatment
For Cohort 2 that contained BTK-inhibitor–naïve patients, Mehta et al. reported the findings [10]. Here, 108 and 77 individuals made up the total and daily groups, respectively. Responses were observed in 70 % and 71 %, respectively, with 15 % and 12 % obtaining CR, respectively (Figure). Partial responses occurred in 56 % and 60 %, respectively. Eighty-four percent and 87 %, respectively, developed regression of their target lesions. Median duration of response was 14.7 and 9.0 months, respectively, and median PFS was 11.1 months in both groups. Median OS had not been reached yet in either group. At 18 months, 69 % and 68 % of patients, respectively, were alive.
Overall, parsaclisib showed clinical activity in both cohorts with r/r MCL. The efficacy of treatment was deemed excellent in the BTK-inhibitor–naïve setting. Here, the authors concluded that parsaclisib represents a potential new option and is a first-in-class PI3Kδ inhibitor in the setting of MCL. In both Cohort 1 and 2, the new agent demonstrated an acceptable safety profile and was generally well tolerated.
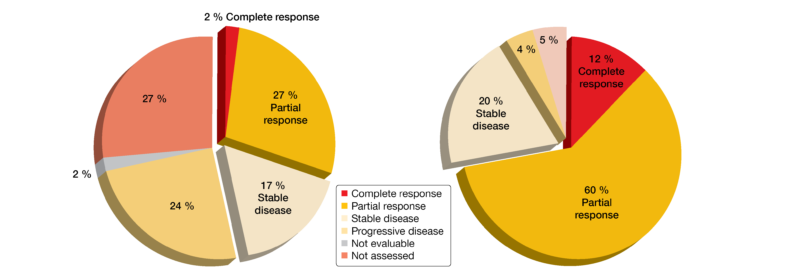
Figure: CITADEL-205: responses obtained with parsaclisib in BTK-inhibitor–pretreated patients (left) and not pretreated patients (right; daily dosing groups)
REFERENCES
- Swerdlow SH et al., The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016; 127(20): 2375-2390
- Vose JM, Mantle cell lymphoma: 2017 update on diagnosis, risk-stratification, and clinical management. Am J Hematol 2017; 92(8): 806-813
- Jain P, Wang M, Mantle cell lymphoma: 2019 update on the diagnosis, pathogenesis, prognostication, and management. Am J Hematol 2019; 94(6): 710-725
- Owen C et al., Review of Bruton tyrosine kinase inhibitors for the treatment of relapsed or refractory mantle cell lymphoma. Curr Oncol 2019; 26(2): e233-240
- Wang M et al., Durable response with single-agent acalabrutinib in patients with relapsed or refractory mantle cell lymphoma. Leukemia 2019; 33(11): 2762-2766
- Wang M et al., Acalabrutinib monotherapy in patients with relapsed/refractory mantle cell lymphoma: long-term efficacy and safety results from a phase 2 study. ASH 2020, abstract 2040
- Jain P et al., Combination of ibrutinib with rituximab in previously untreated older patients with mantle cell lymphoma – a phase II clinical trial. ASH 2020, abstract 2042
- Song Y et al., Long-term safety and efficacy of orelabrutinib monotherapy in Chinese patients with relapsed or refractory mantle cell lymphoma: a multicenter, open-label, phase II study. ASH 2020, abstract 2048
- Zinzani PL et al., Phase 2 study evaluating the efficacy and safety of parsaclisib in patients with relapsed or refractory mantle cell lymphoma previously treated with ibrutinib (CITADEL-205). ASH 2020, abstract 2044
- Mehta A et al., Phase 2 study evaluating the efficacy and safety of parsaclisib in patients with relapsed or refractory mantle cell lymphoma not previously treated with a BTK inhibitor (CITADEL-205). ASH 2020, abstract 1121
© 2020 Springer-Verlag GmbH, Impressum
More posts
PD-1 inhibition and (Non-)Hodgkin lymphoma: promising outcomes in an emerging field
Mediastinal gray zone lymphoma (MGZL) is an extremely rare type of Non-Hodgkin lymphoma with a predominance in young men. This disease exhibits transitional features between nodular sclerosis classical Hodgkin lymphoma (cHL) and primary mediastinal B-cell lymphoma (PMBL). However, compared to PMBL, survival of patients with MGZL is inferior after conventional chemotherapy.
Finding the way among a multitude of targets and regimens
I would like to address two factors here. The first one relates to favorable disease biology. Patients who have mutated immunoglobulin genes or lack TP53 mutations or 17p loss are more likely to experience treatment-free remission. The other main factor is treatment capable of inducing deep remission, which is usually combination therapy. Historically, the fludarabine/cyclophosphamide/rituximab regimen was the gold standard with which patients could achieve deep remissions.
Advancing treatment in patients with mantle cell lymphoma
High relapse rates after standard-of-care regimens in the frontline setting are typical of mantle cell lymphoma (MCL), which is an aggressive, rare, B-cell Non-Hodgkin lymphoma. The second-generation, highly selective BTK inhibitor acalabrutinib has been approved in the US for the treatment of patients with MCL after ≥ 1 prior therapy based on the single-arm, open-label, multicenter, phase II ACE-LY-004 study.
Approaching marginal zone lymphoma from various angles
Approximately 10 % of Non-Hodgkin lymphomas are classified as marginal zone lymphoma (MZL) [1]. This is a heterogeneous malignancy with three main subtypes (i.e., extranodal, nodal, splenic) arising from memory B cells in the marginal zone of secondary lymphoid follicles [2, 3]. Due to its rarity and heterogeneous nature, the optimal therapeutic strategies for patients with MZL have been difficult to define.
Insights from early clinical trials on targeted treatment in B-cell malignancies
Richter’s transformation (RT), which describes transformation of CLL/SLL to diffuse large B-cell lymphoma (DLBCL) or Hodgkin lymphoma, is a rare event occurring in approximately 5–7 % of CLL cases [1]. However, defined standards of care are lacking, and outcomes are generally poor once patients are refractory to rituximab plus chemotherapy.
Management of CLL patients: BTK inhibition and beyond
BTK inhibitors, the Bcl-2 inhibitor venetoclax and anti-CD20 antibodies such as obinutuzumab have dramatically changed the therapeutic landscape of chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL). Ibrutinib, as the first-generation representative of the BTK inhibitor class, is a therapeutic mainstay, although it has notable shortcomings that led to the introduction of second-generation agents.