Early-stage NSCLC: promising (neo)adjuvant approaches
The NEOSTAR trial
Effective treatment options are called for in patients with resectable non-small-cell lung cancer (NSCLC), as more than half of those with stage I to III disease experience relapses [1]. Chen et al. demonstrated in their animal model that tumor PD-L1 upregulation is critical for the spread and survival of metastases [2]. Based on these considerations, several clinical trials are investigating the potential benefits of immunotherapies in the neoadjuvant setting.
The randomized phase II NEOSTAR trial included 44 surgical candidates with stage I to IIIA NSCLC [3]. They were randomized to 3 doses of nivolumab 3 mg/kg on days 1, 15, and 29, or the same nivolumab schedule plus ipilimumab 1 mg/kg on day 1. Surgery was performed within 3 to 6 weeks after the last dose. Major pathological response (MPR), i.e., ≤ 10 % viable tumor cells, was defined as the primary endpoint. It was assumed that nivolumab and/or the combination will produce an MPR rate greater than the one achieved with induction chemotherapy as compared to historical controls. Among the 44 randomized patients, who made up the intent-to-treat (ITT) population, 23 received nivolumab alone, and 21 were treated with nivolumab plus ipilimumab. Thirty-nine patients underwent surgical resection.
Clinical benefits & increased T-cell infiltration
The MPR rate observed in the combination group met the pre-specified trial efficacy boundary. For the ITT population, it was shown that MPRs plus pathological complete responses (pCRs; i.e., 0 % viable tumor cells) occurred in 33 % of patients treated with both nivolumab and ipilimumab (Figure 1). With nivolumab alone, this was 17 %. In the resected population, the combination induced a 44 % MPR plus pCR rate, with pCR accounting for 38 % (MPR plus pCR for nivolumab, 19 %). Overall response rates (ORR) by RECIST according to imaging were 19 % and 22 %, respectively, in the ITT population. One patient in the combination arm (5 %) achieved complete response (CR); in both arms, a total of eight patients (36 %) had partial responses (PRs).
No unacceptable toxicity or increases of perioperative morbidity or mortality were observed. However, the authors noted that nodal immune flares deserve attention in the context of neoadjuvant immunotherapy, as patients might experience seeming radiographic nodal progression due to the emergence of granulomas that need to be distinguished from tumor growth. This is important as potentially curative surgery might be withheld if clinicians fail to differentiate between nodal immune flares and disease progression.
RECIST responses were shown to be positively associated with MPR rates. Elevated baseline PD-L1 expression correlated with radiographic responses and pathological tumor regression. In accordance with the improvement of response rates, immune characterization of surgical samples by flow cytometry revealed that the combined treatment was associated with higher frequencies of CD3-positive tumor-infiltrating lymphocytes as well as tissue resident and effector memory T cells. Moreover, nivolumab plus ipilimumab gave rise to increases of T cell repertoire diversity and reactivity in the tumor.
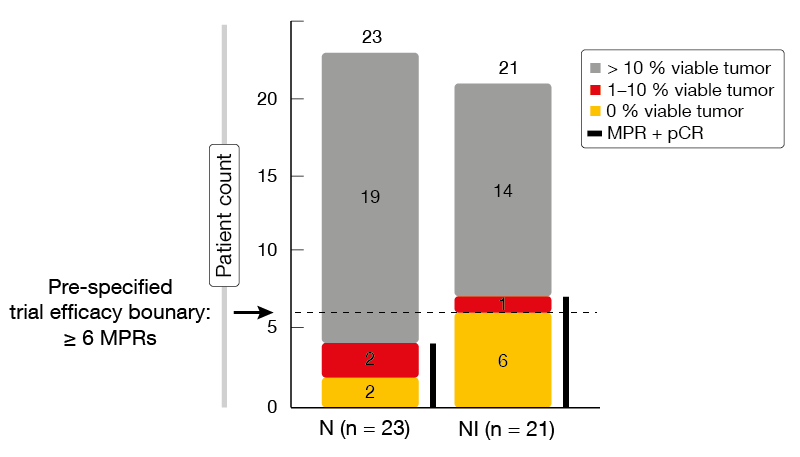
Figure 1: NEOSTAR: pathological response rates obtained with
REFERENCES
- Pignon JP et al., Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol 2008; 26(21): 3552-3559
- Chen L et al., Metastasis is regulated via microRNA-200/ZEB1 axis control of tumour cell PD-L1 expression and intratumoral immunosuppression. Nat Commun 2014; 5: 5241
- Cascone T et al., Neoadjuvant nivolumab or nivolumab plus ipilimumab for resectable non-small cell lung cancer (NSCLC): clinical and correlative results from the NEOSTAR study. J Clin Oncol 37, 2019 (suppl; abstr 8504)
- Kwiatkowski DJ et al., Neoadjuvant atezolizumab in resectable non-small cell lung cancer (NSCLC): interim analysis and biomarker data from a multicenter study (LCMC3). J Clin Oncol 37, 2019 (suppl; abstr 8503)
- Provencio M et al., Neo-adjuvant chemo-immunotherapy for the treatment of stage IIIA resectable non-small-cell lung cancer (NSCLC): a phase II multicenter exploratory study. Final data of patients who underwent surgical assessment (NADIM). J Clin Oncol 37, 2019 (suppl; abstr 8509)
- Kenmotsu H et al., Randomized phase III study of pemetrexed/cisplatin versus vinorelbine/cisplatin for completely resected non-squamous non-small-cell lung cancer. The JIPANG study. J Clin Oncol 37, 2019 (suppl; abstr 8501)
- Tang W et al., EGFR inhibitors as adjuvant therapy for EGFR mutation positive non-small cell lung cancer. J Clin Oncol 37, 2019 (suppl; abstr 8508)
- Khalil M et al., The tumor microenvironment in EGFR-driven loco-regional lung adenocarcinoma can predict higher risk of recurrence. J Clin Oncol 37, 2019 (suppl; abstr 8521)
- Chaft JE et al., Randomized phase II study of adjuvant afatinib for 3 months versus 2 years in patients with resected stage I-III EGFR mutant NSCLC. J Clin Oncol 37, 2019 (suppl; abstr 8507)
- Moding EJ et al., ctDNA for personalization of consolidation immunotherapy in localized non-small cell lung cancer. J Clin Oncol 37, 2019 (suppl; abstr 2547)
© 2019 Springer-Verlag GmbH, Impressum
More posts
New therapeutic options being currently investigated in advanced or metastatic colorectal cancer
Colorectal cancer (CRC) is the second leading cause of cancer death in the United States, and it is the fourth most frequent cancer diagnosis.A current treatment option for RAS and BRAF wild-type (WT) metastatic colorectal cancer (mCRC) is the chemotherapy doublet (FOLFOX/FOLFIRI) with an anti-EGFR monoclonal antibody (cetuximab or panitumumab).
An update and future directions in advanced gastric or gastrointestinal junction cancer (G/GEJC)
With more than 1 million newly diagnosed cases in 2020, gastric cancer (GC) is the fifth most frequent cancer; it was also the third leading cause of cancer-related death worldwide. Gastroesophageal junction (GEJ) cancer concerns a form of gastric cancer developing around the digestive tract where esophagus and stomach connect; in the last years, the prevalence of GEJ constantly increased.
Innovative combinations in esophageal squamous cell carcinoma
Each year, esophageal cancer (EC) is responsible for more than half a million deaths worldwide. Among them, esophageal squamous cell carcinoma (ESCC) accounts for the vast majority (~ 85 %) of EC incidences . At diagnosis, 70 % of ESCC is unresectable [3] and the 5-year survival rate is limited (30 % - 40 %). Patients with advanced or metastatic ESCC have a poor prognosis; their overall survival (OS) after standard first-line chemotherapy is limited to less than a year and other treatment options are scarce.
Novel agents or combinations in recurrent or metastatic nasopharyngeal cancer
Nasopharyngeal cancer (NPC) is a rare malignancy with an incidence of approximately 133,000 annually worldwide, resulting in about 80,000 deaths per year. Whereas early-stage and locally advanced NPC have a good prognosis, treatment of recurrent or metastatic nasopharyngeal cancer is a challenging; it is thus associated with a poor prognosis, especially in patients who have failed two or more lines of systemic therapy, with a median progression-free survival (mPFS) of seven months and median overall survival (mOS) of 22 months.
Preface ASCO Solid Tumor 2022
After 2 years of the COVID-19 pandemic, the Annual Meeting of the American Society of Clinical Oncology (ASCO), was held in Chicago, USA, and virtually from 3rd–7th June 2022.As always, the very much-anticipated event brought leading experts from across the globe together to learn and discuss the groundbreaking updates and scientific advancements which were covered in more than 2,000 abstracts, along with 85 livestream sessions, and more than 2,500 poster presentations.