Genomic testing – becoming part of everyday practice
Prediction of node negativity with a view to sublobar resection
As patients with node-negative early lung cancer might be ideal candidates for sublobar resection, predictors of pathological node-negative disease were investigated in a cohort of patients with clinical stage IA NSCLC [1]. These included 502 patients with adenocarcinoma and 100 with squamous-cell carcinoma from four institutions. The relationship between lymph node status and preoperative factors, such as tumour size according to high-resolution computed tomography (HRCT) and the maximum standardised uptake value (SUVmax) on fluorodeoxyglucose positron emission tomography (FDG-PET/CT), was examined.
In the adenocarcinoma cohort, SUVmax on FDG-PET/CT and tumour size on HRCT may be useful to predict node-negative stage IA lung cancer. When solid tumour size was < 0.8 cm or SUVmax was < 1.5 (N0 criteria), approximately 50 % of patients with stage cT1 disease had no affected lymph nodes (Table). Sublobar resection was shown to be feasible in stage IA tumours that meet N0 criteria, as relapse-free survival and overall survival (OS) did not differ between patients treated with lobectomy or sublobar resection.
For patients with squamous-cell carcinoma, no independent predictive factors for lymph node metastasis were identified. In particular, tumour size on HRCT and SUVmax on FDG-PET/CT were not predictive of lymph node status in IA carcinoma.
IASLC/ATS/ERS classification and benefit from adjuvant therapy
A retrospective study evaluated whether subtypes according to the 2011 International Association for the Study of Lung Cancer (IASLC)/American Thoracic Society (ATS)/European Respiratory Society (ERS) classification are predictive for benefits derived from adjuvant chemotherapy in patients with resected stage IB lung adenocarcinoma [2]. All of these patients had undergone complete resection with mediastinal lymph node dissection or sampling. Adjuvant chemotherapy was not given in a randomised manner, but was used according to the physician’s choice.
Out of 359 patients, 137 (38.2 %) had received adjuvant therapy, which consisted of platinum-based doublet chemotherapy in 54 % of cases. Forty-two percent were treated with oral tegafur-uracil, and 4.4 % received EGFR tyrosine kinase inhibitor therapy. The platinum-based doublet chemotherapy regimens contained docetaxel, vinorelbine and gemcitabine. In the group of patients who were treated with adjuvant chemotherapy, female gender, tumour size of > 3 cm, and a predominantly micropapillary/solid pattern were found significantly more frequently as compared to those who only underwent surgery.
Indeed, tumour size > 3 cm and micropapillary/solid predominant pattern were identified as factors that significantly decreased survival. In patients receiving surgery alone, the lepidic/acinar/papillary predominant pattern was associated with a significantly longer OS (p = 0.027) and disease-free survival (DFS; p = 0.001) compared to the micropapillary/solid predominant pattern. In contrast, in patients treated with adjuvant chemotherapy, neither the micropapillary/solid predominant pattern nor the lepidic/acinar/papillary predominant pattern were predictive of OS and DFS. Interestingly, in patients with the micropapillary/solid predominant subtype, adjuvant platinum-based chemotherapy significantly improved DFS (p = 0.011) and tended to improve OS (p = 0.055) compared to surgery alone (Figure). In contrast, patients with the lepidic/acinar/papillary predominant subtype did not derive any benefit from adjuvant platinum-based chemotherapy.
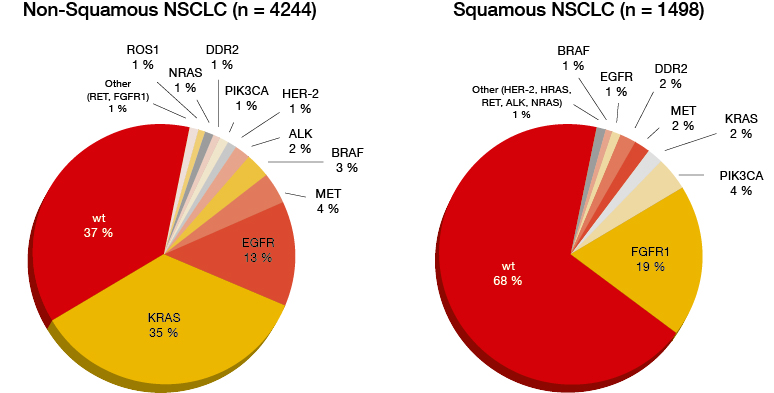
Figure: Gene alterations in non-squamous and squamous NSCLC
The researchers concluded that the IASL/ATS/ERS classification may have a significant predictive value with regard to potential benefits from adjuvant therapy in stage IB lung adenocarcinoma. However, prospective multi-institutional studies and randomised clinical trials are mandatory to further validate these results.
Mutation patterns across lung cancer
The prevalence and clinical association of gene mutations were investigated in the ETOP Lungscape Project, in which 17 centres that are mainly located in Europe participated [3]. A total of 2,709 surgically resected, stage I to III NSCLC patients constituted the Lungscape Tumour Cohort. In the study presented at the ECC, the prevalence of selected cancer-related mutations, their interrelationships, the correlation of the mutation patterns with other molecular alterations, as well as outcome of the patients were determined. Multiplex mutation testing was applied in 1,801 patients, whose median follow-up after surgery was 4.7 years. Gene mutation testing was conducted using Fluidigm technology. The Fluidigm Gene Panel is designed to reveal multiple cancer indications, including for lung cancer. The functionally relevant genes related to lung cancer include EGFR, KRAS, ERBB2, BRAF (V600E/K), PIK3CA (L755P) and AKT1 (E17K). The roles of ERBB2, BRAF, PIK3CA and AKT1 mutations in anti-cancer therapies remain to be established.
In the entire cohort, KRAS was the most frequent mutation (23.1 %), followed by MET (6.8 %), EGFR (5.2 %) and PI3KCA (4.6 %). The other mutations had very low prevalence. According to the histology, adenocarcinoma is associated with a much higher prevalence of KRAS mutations (38.0 %) than squamous-cell carcinoma (6.2 %). For PIK3CA, the distribution was reversed (3.3 % and 6.4 %, respectively). EGFR mutations were more frequent in never smokers than in current or former smokers (19.7 % versus 3.3 %).
KRAS and EGFR mutation prevalence was higher in females, patients with adenocarcinoma, and smaller tumour size. In patients diagnosed with PIK3CA mutation, tumour size tended to be larger, and the histology was predominantly squamous-cell carcinoma. The well-known mutual exclusivity between KRAS mutation and EGFR mutation was confirmed. MET status showed an association with KRAS and EGFR mutations, but not with PIK3CA mutation. The outcome analysis showed no association between relapse-free survival or OS and any of the mutations.
Malignant pleural effusion: Rh-endostatin
Recombinant human endostatin (Rh-endostatin) combined with chemotherapy was assessed in Chinese patients suffering from malignant pleural effusion, both as primary treatment and after failure of previous intra-pleural therapy [4]. Rh-endostatin is a broad-spectrum anti-angiogenesis inhibitor that regulates groups of active proteins involved in angiogenesis, including the expression levels of VEGF-A, FGFR, and HIF-1<. In this trial, Rh-endostatin was administered by means of intracavitary injection together with cisplatin, while the control group received cisplatin only.
The ORR, which was defined as the primary endpoint, was significantly in favour of the combination (76.4 % vs. 55.0 %; p < 0.05). This was accompanied by a significantly greater improvement in Karnofsky performance status (88.0 % vs. 60.0 %; p < 0.05). With regard to AEs, patients receiving Rh-endostatin plus cisplatin experienced higher rates of neutropenia, anaemia, diarrhoea, fatigue and rash, but none of these differences were significant. No grade 3/4 AEs were observed. The authors concluded that the combination has promising efficacy that is superior to cisplatin alone.
REFERENCES
- Kostenko A et al., Broad implementation of next generation sequencing based lung cancer genotyping in clinical routine within a nationwide health care provider network in Germany. ECC 2015, abstract 3006
- Ali SM et al., Comprehensive genomic profiling characterizes the spectrum of non-V600E activating BRAF alterations including BRAF fusions in lung cancer. ECC 2015, abstract 3007
More posts
Optimising treatment in local and regional lung cancer
As patients with node-negative early lung cancer might be ideal candidates for sublobar resection, predictors of pathological node-negative disease were investigated in a cohort of patients with clinical stage IA NSCLC [1]. These included 502 patients with adenocarcinoma and 100 with squamous cell carcinoma from four institutions.
Genomic testing – becoming part of everyday practice
As patients with node-negative early lung cancer might be ideal candidates for sublobar resection, predictors of pathological node-negative disease were investigated in a cohort of patients with clinical stage IA NSCLC [1]. These included 502 patients with adenocarcinoma and 100 with squamous-cell carcinoma from four institutions.
Lung cancer screening: diagnosis in the nick of time
Lung cancer is the leading cause of cancer mortality worldwide. Only 16 % of patients survive for 5 years, compared to 89 % with breast cancer and almost 100 % with prostate cancer. Likewise, only 16 % of patients with lung cancer are diagnosed before the disease has spread (vs. 60 % with breast cancer and 90 % with prostate cancer).
Interview: Immunotherapy has opened up a new avenue of research
The treatment of lung cancer has advanced considerably in the last few years. Which of these advances would you deem most important from the clinical point of view?
Pivotal results and sub-analyses in the field of immunotherapy
Binding of the inhibitory receptor PD-1 to its ligands, PD-L1 and PD-L2, inhibits T-cell responses. This pathway can be exploited by tumours to escape T-cell-induced anti-tumour activity. Therefore, it is a target for antibodies designed to block this mechanism, with the aim of enhancing immune responses.
Interview: Liquid biopsy is a revolution
What changes in practice have been brought about by the recent advances in the treatment of lung cancer?