Approaching squamous-cell carcinoma in a targeted manner
Possible benefit from afatinib
The EGFR mutation status is not routinely examined in NSCLC patients with squamous cell cancer (SCC) histology due to the low incidence of EGFR mutations in these tumours and poor clinical response to first-generation EGFR TKI treatment. Taniguchi et al. retrospectively reviewed 441 consecutive patients in 23 of whom the EGFR mutation status was assessed, in order to explore the clinical features of SCC with sensitive EGFR mutation, and to select the optimal indications for afatinib treatment [1].
Five patients tested positive for sensitising EGFR mutations (exon 19 deletion and L858R mutation). All of these were female and never smokers. Four had normal lung function, and only one had underlying emphysema/ fibrosis. Four patients received TKI treatment; gefitinib and afatinib were administered in two patients each. While gefitinib did not elicit any clinical responses, the afatinib-treated patients responded well, achieving partial remissions. At the time of the analysis, they were still alive, whereas the gefitinib-treated patients had died. In their conclusion, the authors noted that patients with SCC might benefit from afatinib treatment. Patient selection using baseline characteristics could contribute to identifying a population with greater sensitivity to afatinib.
ErbB mutation status counts
A genetic analysis of patients who participated in the LUX-Lung 8 trial was conducted with the aim of establishing the frequency of ErbB family mutations and the patient outcomes according to mutation status [2]. LUX-Lung 8 compared second-line afatinib and erlotinib in patients with SCC, revealing significant benefits in the afatinib-treated group [3]. Tissue samples were retrospectively selected and enriched for patients with PFS ≥ 2 months to reflect a range of responsiveness to EGFR TKIs. The tumour genetic analysis subset consisted of 245 patients, 132 of whom had received afatinib. This cohort was representative of the overall LUX-Lung 8 population; both PFS and OS favoured afatinib over erlotinib.
As the analysis showed, 53 patients (21.6 %) had at least one ErbB family mutation. In both wild-type and ErbB-mutation-positive cohorts, afatinib gave rise to superior PFS (Figure) and OS compared to erlotinib, although this effect was more pronounced in the mutant group. For erlotinib, on the other hand, PFS and OS did not differ according to ErbB mutation status. OS achieved with afatinib was 10.6 months in the ErbB-mutation-positive group and 8.1 months in the wild-type population.
The accentuated benefit of afatinib over erlotinib in patients with ErbB mutations did not appear to be driven by EGFR, as the largest benefits were observed with HER3, HER4, and, in particular, HER2 mutations. No apparent correlation emerged between ErbB amplification or EGFR expression and clinical outcomes. The authors concluded that next-generation sequencing might help to identify patients with SCC of the lung who could derive additional benefit from afatinib or erlotinib. The role of ErbB mutations, particularly HER2 mutations, as predictive markers for afatinib warrants further evaluation.
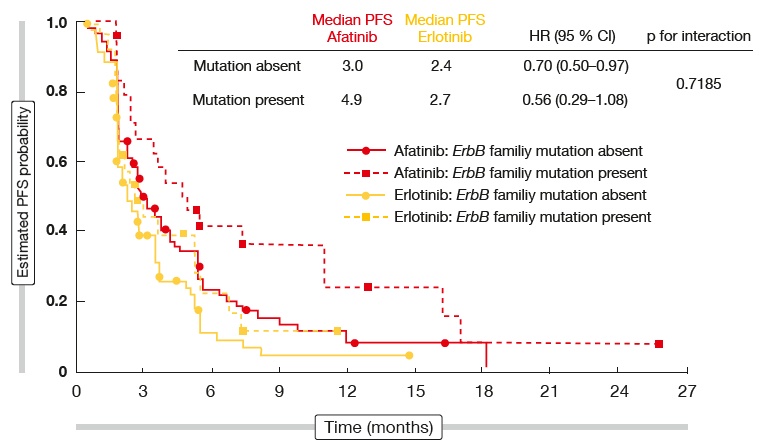
Figure: Progression-free survival obtained with afatinib vs. erlotinib in LUX-Lung 8 according to ErbB family mutation status
Ongoing trial of afatinib plus pembrolizumab
Preclinical evidence suggests that both the immune microenvironment and tumour expression of PD-L1 can be modulated by EGFR signaling in EGFR-mutant NSCLC [4, 5]. Afatinib is currently being tested in combination with the anti-PD-1 antibody pembrolizumab based on the assumption that concurrent inhibition of the EGFR and PD-1 pathways represents a rational and promising approach for treatment of SCC of the lung, to improve responses and delay the onset of resistance [6]. Recruitment into the open-label, single-arm phase II trial named LUX-Lung IO/ KEYNOTE 497 started in October 2017 in the USA, Spain, France, South Korea, and Turkey (NCT03157089). Objective response has been defined as the primary endpoint. The target population comprises 50 to 60 patients.
REFERENCES
- Taniguchi Y et al., The clinical features of squamous cell lung carcinoma with sensitive EGFR mutations. WCLC 2017, P2.03-017
- Goss GD et al., Impact of ERBB mutations on clinical outcomes in afatinib- or erlotinib-treated patients with SqCC of the Lung. WCLC 2017, P3.01-043
- Soria J-C et al., Afatinib versus erlotinib as second-line treatment of patients with advanced squamous cell carcinoma of the lung (LUX-Lung 8): an open-label randomised controlled phase 3 trial. Lancet Oncol 2015; 16: 897-907
- Chen N et al., Upregulation of PD-L1 by EGFR activation mediates the immune escape in EGFR-driven NSCLC: implication for optional immune targeted therapy for NSCLC patients with EGFR mutation. J Thorac Oncol 2015; 10: 910-923
- Akbay EA et al., Activation of the PD-1 pathway contributes to immune escape in EGFR-driven lung tumors. Cancer Discov 2013; 3: 1355-1363
- Riess AJ et al., Afatinib in combination with pembrolizumab in patients with stage IIIB/IV squamous cell carcinoma of the lung. WCLC 2017, P2.04-010
More posts
Chemotherapy: new approaches, new settings
Current guidelines recommend postoperative platinum-based chemotherapy in completely resected NSCLC with nodal involvement (stage II-IIIA). However, survival outcomes remain limited, and compliance is lower than for adjuvant therapy in other neoplasms. There are no direct comparisons between different chemotherapy regimens.
Malignant mesothelioma: recent data on nintedanib and checkpoint inhibitors
Malignant pleural mesothelioma (MPM) is an aggressive tumour that, if left untreated, shows a median survival of 7–9 months. The front-line standard treatment for patients with unresectable MPM consists of combination doublet therapy with cisplatin and pemetrexed, which yields a median OS of approximately 1 year.
Approaching squamous-cell carcinoma in a targeted manner
The EGFR mutation status is not routinely examined in NSCLC patients with squamous cell cancer (SCC) histology due to the low incidence of EGFR mutations in these tumours and poor clinical response to first-generation EGFR TKI treatment. Taniguchi et al. retrospectively reviewed 441 consecutive patients in 23 of whom the EGFR mutation status was assessed, in order to explore the clinical features of SCC with sensitive EGFR mutation, and to select the optimal indications for afatinib treatment.
Immunotherapy: novel biomarkers on the horizon & news from pivotal trials
Only limited treatment options are available for patients with recurrent small-cell lung cancer (SCLC). The CheckMate 032 trial evaluated the anti-PD-1 antibody nivolumab with or without the anti-CTLA-4 antibody ipilimumab in a PD-L1–unselected cohort of SCLC patients who had received at least one prior platinum-based chemotherapy regimen.
Taking anti-EGFR drug treatment further: later lines
Acquired resistance usually follows first-line EGFR TKI therapy, with the gatekeeper T790M mutation being the most common mechanism. The third-generation irreversible EGFR TKI osimertinib has been licensed for the treatment of patients whose tumours have been shown to carry this mutation. Retrospective data presented by Tan et al. demonstrated the activity of later-line osimertinib in 52 patients who participated in an early access program in Singapore.
“We are making steady progress toward better lung cancer control”
In a way, synergy is another expression for the multidisciplinary team approach, but the term ,multidisciplinary’ is not necessarily restricted to medical doctors. It also includes nursing staff and others such as the supportive care team, including the rehabilitation team and patient advocates. At the same time, the bottom line of that concept is having the patient at the centre of the overall care plan.