Deepening and extending response to treatment in Multiple Myeloma
Follow-up on long-term responders in the DREAMM-7 trial
The open-label, randomized phase III trial DREAMM-7 compared the safety and efficacy of two combination treatments, BVd (Belantamab-Mafodotin, Bortezomib, dexamethasone) and DVd (Daratumumab + Vd) in patients with refractory and relapsing Multiple Myeloma (R/R MM) who have received ≥ 1 line of treatment (LOT). Belantamab-Mafodotin is a novel antibody-drug conjugate (ADC) targeting the B-cell maturation antigen (BCMA) in myeloma cells. Patients in the BVd group experienced deeper responses and higher rates of minimal residual disease negativity (MRD-) compared to those in the DVd group. Total MRD rates were 25% vs. 10%, while MRD6 rates (1 cancer cell among 106 cells in peripheral leukocytes) were 16% vs. 4% [1].
At ASH 2025, Hungria et al. and Mateos et al. presented new data, following up on long-term responders and patients who achieved MRD- in the DREAMM-7 trial. Patients who responded for at least 36 months were considered long-term responders (LTR). In the BVd arm, 72% of patients achieved at least a complete response (CR) compared to 57% in the DVd arm. Response durability was strongly associated with the depth of response. In the BVd vs. DVd treatment arms, 75% vs. 70% of LTRs who achieved ≥ CR and 73% vs. 58% of LTRs who achieved ≥ very good partial response (VGPR) also reached MRD- status [2]. MRD- was achieved faster (11.14 vs. 17.02 months) and sustained significantly longer with BVd vs. DVd, reaching 12-month-rates of 57.4% vs. 42.3% in patients with ≥ CR and 14.4% vs. 4.4% overall. Among MRD- patients, the BVd arm had a higher proportion of patients with unfavorable prognostic markers, with 40% vs. 27% having high-risk cytogenetics and 37% vs. 9% having had ≥ 2 LOT. This suggests BVd can induce deep responses in high-risk patients more effectively than DVd [3].
The safety profiles in the MRD- and long-term responder groups were consistent with the primary analysis and similar between treatment arms, thus confirming the established efficacy of the BVd regimen in patients with R/R MM [2,3].
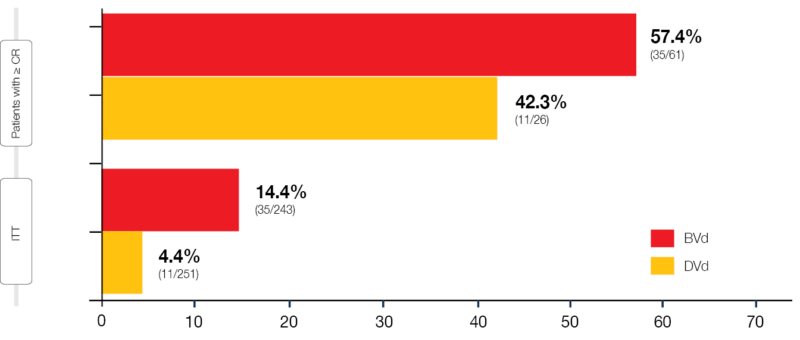
Figure 1: Rate of patients achieving MRD negativity with BVd and DVd in DREAMM-7. ITT, intention-to-treat.
Long-term follow-up in DREAMM-8
DREAMM-8 is a phase III, open-label, randomized clinical trial that evaluated the safety and efficacy of the BPd (Belantamab-Mafodotin, Pomalidomide and dexamethasone) vs. the PVd (Pomalidomide, Bortezomib and dexamethasone) treatment regimen in patients with R/R MM after ≥1 line of treatment. At a median follow-up of 21.8 months, BPd demonstrated superior efficacy over PVd in terms of progression-free survival (PFS) (12-month PFS rate: 71% vs. 51%) [4].
A presentation by Trudel et al. showed long-term follow-up data (median: 35.8 months) from DREAMM-8, including efficacy and safety findings. Deep responses to treatment occurred more frequently with BPd vs. PVd (VGPR: 63% vs. 39%; CR: 43% vs. 17%) and more patients achieved MRD- (28% vs. 6%; 64% vs. 36% in patients who achieved CR). CR-based MRD- was sustained for ≥12 months in 15% vs. 3% of the intention-to-treat populations. This resulted in a markedly longer median progression-free survival (mPFS; 32.6 months vs. 12.5 months), which persisted into the subsequent antimyeloma therapy (mPFS2: 47.1 months vs. 21.7 months).
The updated safety data was consistent with the primary analysis, confirming the previously established manageable safety profile [4].

Figure 2: Progression-free survival with BPd vs. PVd after subsequent antimyeloma therapy (PFS2) in DREAMM-8. CI, confidence interval; HR, hazard ratio; NR, not reached.
Treatment efficacy and Ocular Events in DREAMM-9
The phase I, randomized clinical trial DREAMM-9 is a dose-finding and schedule-evaluation study investigating Belantamab-Mafodotin + VRd (BVRd) in patients with transplant-ineligible, newly diagnosed MM (TI NDMM). Data from three cohorts with dosage regimens of 1.9 mg/kg three times in a four-week cycle (Q3/4W), 1.9 mg/kg Q6/Q8W, and 1.4 mg/kg Q6/8W were presented at the ASH 2025 congress. In the respective cohorts, rates of ≥ CR were at 75%, 92% and 91%, indicating poorer response at the most intensive dosing regimen; rates of stringent CR, however, were 50%, 33% and 27%, and MRD negativity occurred in 100%, 67% and 45% of participants with ≥ CR, respectively [5].
Intensity of treatment correlated with the occurrence of adverse events (AEs), e.g., Grade (Gr) 3/4 events related to Belantamab-Mafodotin (67% vs. 25% vs. 33%). This, however, did not apply to the rate at which at least one treatment drug was discontinued (50% vs. 42% vs. 50%). Interestingly, ocular examination findings (OEFs) Gr ≥ 2, especially bilateral decrease in best corrected visual acuity (BCVA) to 20/50, did not occur at increased rates with higher treatment intensity (50% vs. 50% vs. 50%). Ocular events were managed by dose delays and schedule extensions and resolved for the most part (resolution of first decrease in BCVA to 20/50 or worse: 100% vs. 100% vs. 67%) [5].
To conclude, these data indicate that the BVRd treatment regimen was highly efficacious for patients with NDMM, resulting in high MRD- rates that were strong predictors of long-term response. The authors concluded that strategies for mitigating ocular events remained a priority.

Figure 3: Response rates in three DREAMM-9 cohorts. (s)CR, (stringent) complete response; ORR, objective response rate; Qx/Wy; x times in a y week cycle; (VG)PR, (very good) partial response.
Teclistamab + Daratumumab superior to DVd/DPd combinations: MajesTEC-3
MajesTEC-3 is a phase III, randomized clinical trial, comparing Teclistamab + Daratumumab (Tec + Dara) to Dara + Dexamethasone and Bortezomib (DVd) or Pomalidomide (DPd) by investigator’s choice in patients with R/R MM who had 1‑3 LOT. Tec is a bispecific antibody targeting the B-cell maturation antigen (BCMA) and CD3, while Dara is an anti-CD38 monoclonal antibody.
At the primary analysis presented by Mateos et al., MajesTEC-3 met its primary PFS endpoint, achieving a 36-month rate of 83.4% vs. 29.7% in the DVd/DPd treatment arm. This advantage was seen in all analyzed patient subgroups, including patients ≥ 75 years, with prior anti-CD38 exposure, high-grade disease and high-risk cytogenetics. Importantly, the curve reached a plateau after 6-12 months. Tec-Dara led to CR in 81.8% vs. 32.1% of patients, and 58% vs. 17.1% achieved MRD- status. This translated into a substantial overall survival (OS) benefit, with 83.3% vs. 65% of patients still alive after 36 months [6].
The most common adverse events were neutropenia (any Gr: 78.4%; Gr 3/4: 75.6%) and cytokine release syndrome (CRS; any Gr: 60.1%; Gr 3/4: 0%). Three patients (1.1%) experienced immune effector cell-associated neurotoxicity (ICANS), one of which had Gr 4 ICANS, which led to discontinuation of Teclistamab. All CRS and ICANS events have been resolved. Rates of treatment discontinuation (4.6% vs. 5.5%) and fatal treatment-emergent adverse events (TEAEs; 7.1% vs. 5.9%) were comparable between treatment arms. Most TEAE-related deaths in the Tec-Dara group were associated with infection (4.6% total).
The authors conclude that the plateauing PFS curve suggests Tec-Dara has the potential to be a functional cure, with its CRS profile enabling its adoption as a new standard of care (SOC) for the second line (2L) and following lines [6].

Figure 4: Progression-free survival in the Tec-Dara vs. DPd/DVd treatment arms, MajesTEC-3 clinical trial. CI, confidence interval; HR, hazard ratio; NR, not reached.
In-patient CAR-T cell generation leads to MRD- outcome: inMMyCAR study
A new in vivo gene therapy, KLN-1010, generates anti-BCMA CAR-T cells in patients. Harrison et al. reported preliminary findings from the first-in-human, phase I, inMMyCAR trial in patients with R/R MM. KLN‑1010 is based on lentiviral particles, eliminating the need for ex vivo cultivation and lymphodepletion before administration, thereby simplifying logistics and reducing time and financial burden [7].
KLN-1010 demonstrated greater anti-myeloma activity vs. ex vivo generated CAR-T cell products in mice and high specificity for T-cells in animal models. The inMMyCAR trial is a dose-escalation and expansion trial with three dose levels and ~20 study participants. The initial four patients showed CAR-T cell expansion and persistence for at least one month and memory T-cell formation. All patients achieved MRD- status one month after treatment and showed continuously decreasing levels of serum free light chain, monoclonal protein spike and soluble BCMA.
Among this small number of patients, no events of ICANS, delayed neurotoxicity, or CRS Gr ≥ 3 were recorded. The authors report a favorable safety profile compared to ex vivo CAR-T cell products.
In conclusion, KLN-1010 has the potential to become the first available off-the-shelf CAR-T cell therapy if the safety findings from this phase I trial are confirmed, and responses are durable in continued follow-up and later phase trials.
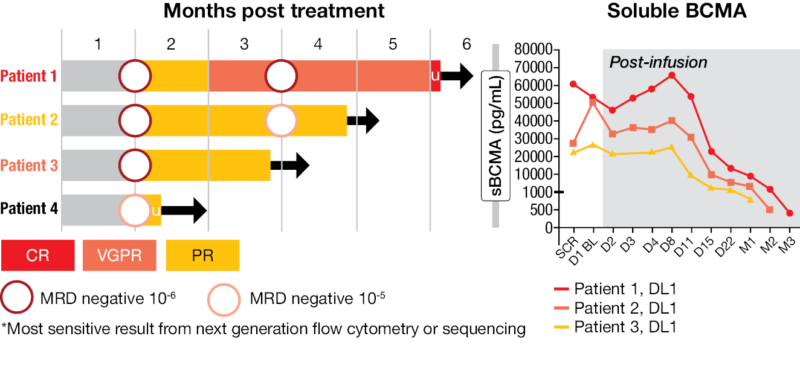
Figure 5: Ongoing responses in the four initial patients treated with KLN-1010 in the inMMyCAR trial. CR, complete response; DL, dose level; MRD, minimal residual disease; (VG)PR, (very good) partial response; sBCMA, soluble B-cell maturation antigen.
REFERENCES
- Hungria V, Robak P, Hus M, et al. Belantamab Mafodotin, Bortezomib, and Dexamethasone for Multiple Myeloma. N Engl J Med 2024;391:393–407. https://doi.org/10.1056/nejmoa2405090.
- Hungria V, Robak P, Hus M, et al. Long-term responders from the Phase 3 dreamm-7 study of belantamab mafodotin plus bortezomib and dexamethasone vs daratumumab plus bortezomib and dexamethasone in Relapsed/Refractory multiple myeloma. Blood 2025;146:2262–2262. https://doi.org/10.1182/blood-2025-2262.
- Mateos M-V, Robak P, Hus M, et al. Patients with Relapsed/Refractory multiple myeloma who achieved sustained minimal residual disease negativity in the dreamm-7 trial. Blood 2025;146:2265–2265. https://doi.org/10.1182/blood-2025-2265.
- Trudel S, Beksac M, Pour L, et al. Deep responses and durable outcomes in patients treated with belantamab mafodotin plus pomalidomide and dexamethasone from long-term follow-up of the Phase 3 dreamm-8 study. Blood 2025;146:2264–2264. https://doi.org/10.1182/blood-2025-2264.
- Usmani S, Mielnik M, Alonso Alonso A, et al. Belantamab mafodotin (belamaf) in combination with bortezomib, lenalidomide, and dexamethasone (VRd) for patients (pts) with transplant-ineligible (TI) newly diagnosed multiple myeloma (NDMM): A focus on treatment efficacy and management/
resolution of ocular events in the Phase 1 dreamm-9 study. Blood 2025;146:5840–5840. https://doi.org/10.1182/blood-2025-5840. - Mateos M-V, Bahlis N, Perrot A, et al. Phase 3 randomized study of teclistamab plus daratumumab versus investigator’s choice of daratumumab and dexamethasone with either pomalidomide or Bortezomib (DPd/DVd) in patients (Pts) with relapsed refractory multiple myeloma (RRMM): Results of
majestec-3. Blood 2025;146:LBA-6-LBA-6. https://doi.org/10.1182/blood-2025-LBA-6. - Harrison S, Ho PJ, Lim S-L, et al. Minimal residual disease (MRD)-negative outcomes following a novel, in vivo gene therapy generating anti–B-cell maturation antigen (BCMA) chimeric antigen receptor (CAR)-T cells in patients with relapsed and refractory multiple myeloma (RRMM): Preliminary
results from inMMyCAR, the first-in-human phase 1 study of KLN-1010. Blood 2025;146:LBA-1-LBA-1. https://doi.org/10.1182/blood-2025-LBA-1.
© 2026 Springer-Verlag GmbH, Impressum
More posts
A PARADIGM shift in newly diagnosed fit AML
Standard initial treatment for acute myeloid leukemia (AML) patients varies based on age and fitness. Typically, younger and fit patients, under 65 years old, receive intensive induction chemotherapy (IC), commonly known as the “7+3” regimen, which consists of cytarabine and an anthracycline, followed by consolidation therapy, allogeneic stem-cell transplantation (HCT), or a combination of both.
New BTK modalities in B-cell malignancies
Targeted agents such as Bruton tyrosine kinase inhibitor (BTKi; e.g., ibrutinib) and B-cell lymphoma-2 inhibitors (BCL2i) have emerged for the treatment of Chronic Lymphocytic Leukemia (CLL).
Deepening and extending response to treatment in Multiple Myeloma
The open-label, randomized phase III trial DREAMM-7 compared the safety and efficacy of two combination treatments, BVd (Belantamab-Mafodotin, Bortezomib, dexamethasone) and DVd (Daratumumab + Vd) in patients with refractory and relapsing Multiple Myeloma (R/R MM) who have received ≥ 1 line of treatment (LOT).
Preface – ASH 2025
Out of the 8,200 abstracts accepted for the ASH 2025 annual congress, we highlight several key abstracts that discuss targeted treatment strategies for lymphoid and myeloid malignancies, especially the high-impact ones showcased in the late-breaking abstract and plenary sessions.