New BTK modalities in B-cell malignancies
Fixed-duration versus continuous targeted treatment for previously untreated CLL
Results from the CLL17 trial (NCT04608318) presented by Othman Al-Sawaf [1].
Targeted agents such as Bruton tyrosine kinase inhibitor (BTKi; e.g., ibrutinib) and B-cell lymphoma-2 inhibitors (BCL2i) have emerged for the treatment of Chronic Lymphocytic Leukemia (CLL). One of the approved first-line treatments for patients with CLL is the time-limited combination of venetoclax, a first-generation BCL2i, with the anti-CD20 antibody obinutuzumab.
Currently, treatment paradigms can be classified into two categories: continuous BTKi or fixed-duration regimens combining BCL2i with a CD20 antibody or BCL2i with BTKi. These two paradigms were compared with chemo-immunotherapy; however, a direct comparison between them is lacking.
In this prospective, randomized, investigator-initiated, phase III trial, Al-Sawaf et al. tested which of these targeted agents and regimens had the longest PFS and how they compared under randomized testing. For this purpose, they designed the trial comparing continuous ibrutinib (I) monotherapy to fixed-duration venetoclax plus obinutuzumab (VO) and fixed-duration venetoclax plus ibrutinib (VI) for CLL. The hypothesis was to test the noninferiority of VO vs. I and of VI vs. I, with PFS as the primary endpoint.
Patients were randomized to receive,
- ibrutinib continuously until intolerance or progression (n = 301), or
- fixed-duration venetoclax plus obinutuzumab for 6 cycles (28 days each) followed by 6 additional cycles of venetoclax monotherapy (n = 303), or
- fixed-duration venetoclax plus ibrutinib (VI, n = 305), initiated with a 3-cycle ibrutinib lead-in, followed by 12 cycles of VI.
The results revealed that 3-year PFS was 81.0% for I, 79.4% for VI and 81.1% for VO. In conclusion, venetoclax plus obinutuzumab and venetoclax plus ibrutinib were non-inferior in investigator-assessed PFS compared with continuous ibrutinib and can be considered as the preferred treatment option for patients with previously untreated CLL. Considerations for treatment, such as the ongoing follow-up and infection control, should be taken into account, and it should be noted that PFS may not be the only clinically relevant endpoint for CLL.
![Figure 1: Progression-free survival (%) results for ibrutinib (l), venetoclax plus obinutuzumab (VO), and venetoclax plus ibrutinib (VI) groups from the CLL17 trial [2]. CI, confidence interval; HR, hazard ratio.](https://memoinoncology.com/wp-content/uploads/2026/04/ash_2025_b-cell-malignancies_1-800x469.png)
Figure 1: Progression-free survival (%) results for ibrutinib (l), venetoclax plus obinutuzumab (VO), and venetoclax plus ibrutinib (VI) groups from the CLL17 trial [2]. CI, confidence interval; HR, hazard ratio.
Pirtobrutinib vs. bendamustine plus rituximab (BR) in patients with CLL/SLL
First results from the BRUIN CLL-313 (NCT05254743) trial examining a non-covalent BTKi in untreated patients presented by Wojciech Jurczak (2025) [3].
Pirtobrutinib is a highly selective, non-covalent (nc) BTKi. While covalent BTKi have significantly improved PFS for untreated patients with CLL, there are no phase III data assessing an ncBTKi.
In this global, open-label, randomized phase III study, the efficacy and safety of pirtobrutinib were evaluated. Pirtobrutinib was compared vs. bendamustine plus rituximab (BendaR), which is a common frontline chemoimmunotherapy for patients with previously untreated CLL or small lymphocytic lymphoma (SLL) lacking a 17p deletion/TP53 mutation.
A total of 282 patients were randomized 1:1 to receive continuous pirtobrutinib monotherapy (200 mg once daily) or 6 cycles of BendaR. The trial’s primary endpoint was PFS assessed by an independent review committee (IRC). A stratified log-rank test was employed to compare PFS using a two-sided alpha threshold of 0.05.
The results demonstrated that pirtobrutinib significantly improved PFS compared with BendaR at a median follow-up of 28.1 months (HR: 0.199; 95% CI: 0.107-0.367; p < 0.0001).
Furthermore, in this trial, pirtobrutinib was well tolerated, consistent with its known safety profile, with low rates of discontinuation and atrial fibrillation/flutter. Overall, pirtobrutinib demonstrated statistically significant superiority over BendaR in IRC-assessed PFS in treatment-naïve CLL/SLL. It should be noted that, at the time of publication [4], this was the third positive phase III study of pirtobrutinib in patients with CLL/SLL, and future research is needed to examine outcomes of covalent BTKi after ncBTKi to address sequencing questions.

Figure 2: Progression-free survival for pirtobrutinib and bendamustine plus rituximab in the BRUIN CLL-313 study.
Sustained efficacy of zanubrutinib vs. bendamustine + rituximab in TN SLL/CLL
6-year follow-up in the Phase III SEQUOIA study (NCT03336333) presented by Constantine Tam (2025) [5].
SEQUOIA is a global phase III, open-label, randomized study that investigated zanubrutinib, a next-generation covalent BTKi with potentially improved selectivity as compared to ibrutinib. The study included patients with treatment-naïve (TN) CLL/SLL with or without the del(17p) mutation. In this poster session at the ASH 2025 congress, updated efficacy results from the SEQUOIA study, with a median long-term follow-up of approximately 6 years, were presented.
The primary goal was to compare the efficacy of zanubrutinib vs. chemoimmunotherapy with bendamustine and rituximab.
Participants were randomized 1:1 to receive zanubrutinib (Arm A, n = 241) or bendamustine plus rituximab (Arm B, n = 238). Neither Arm A nor Arm B patients had del(17p). Zanubrutinib was administered at a dose of 160 mg twice daily (BID) until unacceptable toxicity or end of the study. Bendamustine plus rituximab was administered for a maximum of 6 cycles.
Participants in Arm C (n = 111) had del(17p), and all patients in Arm C received zanubrutinib without randomization. As a side note, Arm C might represent the largest collection of patients with del(17p) receiving frontline treatment.
Additionally, the PFS rate in Arm C when adjusted for COVID-19 was 65% (95% CI, 54.3-73.5). At 72 months, 83% of patients in Arm C (95% CI, 73.6-88.6) had not yet initiated subsequent treatment. Thus, in patients with del(17p), zanubrutinib may improve the historically poor prognosis.
The safety profile of zanubrutinib was consistent with prior studies, and fewer patients treated with zanubrutinib (n = 27) required subsequent treatment as compared to patients treated with bendamustine plus rituximab (n = 84, including 67 who crossed over).
In conclusion, at a 6-year long-term follow-up, zanubrutinib continues to demonstrate robust efficacy and sustained superiority over bendamustine plus rituximab, including among patients with del(17p) mutations.
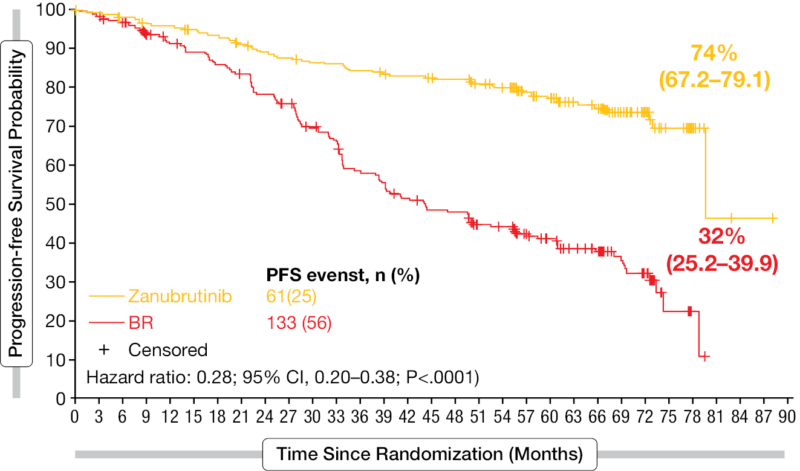
Figure 3: Progression-free survival for zanubrutinib (Arm A) and bendamustine plus rituximab (BR; Arm B). The graph represents results in patients without the del(17p) mutation. CI, confidence interval.
Symptom-Based Progression-Free Survival (S-PFS) as a Patient-Centric Endpoint in CLL/ SLL
In this talk during the ASH 2025 congress, the symptom-based PFS results for the ALPINE trial were presented by Jennifer Brown (2025) [6].
Advances in BTKi have improved the treatment landscape for CLL/SLL. Given this, there is a need for patient-focused approaches and outcome measures to complement traditional endpoints, such as PFS. In this patient-reported outcome (PRO)- focused presentation, the association between longitudinal deterioration in disease-specific symptoms and time to disease progression (defined as PFS events) was evaluated.
For context, the ALPINE trial included patients with relapsed/refractory (R/R) CLL/SLL with ≥1 prior treatment (N = 652) who were randomized in a 1:1 stratified fashion in two groups: zanubrutinib 160 mg BID or ibrutinib 420 mg once daily. Treatment was continued until disease progression or unacceptable toxicity. As evidenced by prior research, improved PFS in patients with R/R CLL treated with zanubrutinib compared with ibrutinib has been observed.
For the purpose of assessing the association between PROs and PFS events, the EORTC-QLQ-C30 questionnaire was used as a PRO instrument. Deterioration was classified as ≥10-point worsening from baseline, and CLL-related outcomes (fatigue, nausea/vomiting, insomnia, and pain) were considered.
A joint model framework combining mixed-effects logistic regression (to estimate the probability of longitudinal symptom deterioration) and Cox proportional hazards regression (to estimate time to investigator-assessed PFS) served as the basis for statistical analysis. The hazard ratio (HR) of >1 indicated an increase in hazard of disease progression when a PRO worsening event is observed. In other words, HR >1 would indicate if symptom worsening predicts the risk of earlier disease progression.
These findings support an association between worsening patient-reported symptoms (particularly increased fatigue, insomnia, and nausea/vomiting) and disease progression. In conclusion, future studies could develop symptom-based PFS to demonstrate treatment effectiveness.

Figure 4: Association parameter indicating an increase in hazard of disease progression when a PRO worsening event for CLL-related symptom domains is observed; calculated with the joint model framework.
Sonrotoclax combination with obinutuzumab continued to demonstrate safety and efficacy in TN CLL
The time-limited combination of venetoclax and obinutuzumab (Ven + Obi) as a first-line therapy for patients with CLL has resulted in a high rate of undetectable MRD and extended PFS, but its use may be constrained by toxicity [7]. Sonrotoclax (BGB-11417), a next-generation BCL2i, is a more selective and pharmacologically potent inhibitor of BCL2 than venetoclax, with a shorter half-life and no drug accumulation [8]. Marc Hoffmann shared the initial results from a cohort of the Phase I/Ib BGB-1147-101 study evaluating sonrotoclax (Sonro) + Obi in TN CLL patients, which used MRD status to guide treatment discontinuation [9].
The conventional dosing of Obi (6 cycles, 1000 mg) was followed. Obi monotherapy was initiated one cycle before the start of Sonro. Sonro was administered orally QD, with ramp-up to target doses of 160 or 320 mg until PD, unacceptable toxicity, or uMRD4 (<1 CLL cell per 10,000 leukocytes [<0.01%]) in peripheral blood by next-generation sequencing (NGS) after 15 treatment cycles. Only data for Sonro 320 mg + Obi were discussed, as data for Sonro 160 mg + Obi were still immature and were presented only for reference.
Patients enrolled in the study had a median age of 62 years, with 65% male. Approximately 10% had del(17p) or TP53 mutations, and approximately 60% had unmutated IGHV status.
The drug combination was generally well tolerated, with most TEAEs being low-grade. The most common Gr ≥3 TEAEs were neutropenia and thrombocytopenia; neutropenia was not linked to serious infections, and thrombocytopenia did not cause major bleeding. There were no TEAE-related deaths, and no treatment discontinuations related to Sonro. Two cases of laboratory tumor lysis syndrome were observed during the Obi ramp-up, but none occurred during the Sonro ramp-up.
An ORR of 94% and a CR/CRi rate of 40% were observed. During the median study follow-up of 12.3 months, there were two episodes of Richter’s transformation in the Sonro 320 mg cohort, both of which occurred early in cycle 2 and cycle 6. The estimated 18-month PFS rate was 94.3% (95% CI: 83.5%-98.1%).
All patients who reached cycle 15 with an NGS sample analyzed achieved at least uMRD5 and discontinued therapy as defined per protocol. Approximately 90% of patients achieved uMRD6, and all patients remained in remission, with a median time off treatment of 7.2 months (range: 1.7-14.4 months).
In conclusion, the combination of Sonro + Obi was well tolerated and showed potent activity in patients with TN CLL. A registrational phase III study (CELESTIAL-RRCLL, BGB-11417-303) assessing this combination is currently recruiting patients with relapsed/refractory CLL.

Figure 5: MRD status in sonrotoclax 320 mg cohort at the end of treatment cycle 15 per NGS. C, Cycle; (u)MRD, (undetectable) minimal residual disease; PD, progressive disease.
Sonrotoclax is effective in heavily pretreated patients with MCL
Sonrotoclax is a 2nd generation BCL2i with higher affinity and better selectivity for its target compared to venetoclax. The BGB-11417-201 phase I/II dose escalation trial investigates the safety and efficacy of sonrotoclax (160 mg QD -> 320 mg QD) in patients with mantle cell lymphoma (MCL) who relapsed after ≥1 line of CD20-based therapy and ≥1 line of BTK inhibition but no previous BCL2i exposure.
Of 125 patients enrolled in the trial, 115 received sonrotoclax 320 mg QD. No dose-limiting toxicities (DLTs) were observed. 42 patients (36.5%) experienced TEAEs, mostly infections. In 31 patients (27%), TEAEs led to treatment modifications, including 31 temporary interruptions and one dose reduction. The most common Gr ≥3 TEAEs (≥5%) were neutropenia (19.1%), thrombocytopenia (9.6%), anemia (7.8%), infections (16.5%) and tumor lysis syndrome (TLS) (7.0%).
The objective response rate (ORR; PR + CR) at the recommended phase 2 dose (RP2D) of 320 mg QD was 52.4%, and the CR rate was 15.5% at a median follow-up of 14.2 months. All subgroups with ≥5 patients showed an ORR benefit relative to the 30% historical control. Patients who responded to treatment remained in response for a median of 15.8 months, yielding an mPFS of 6.5 months. Median OS was not reached [10].
In summary, sonrotoclax demonstrated significant efficacy with good tolerability in a heavily pretreated patient population.
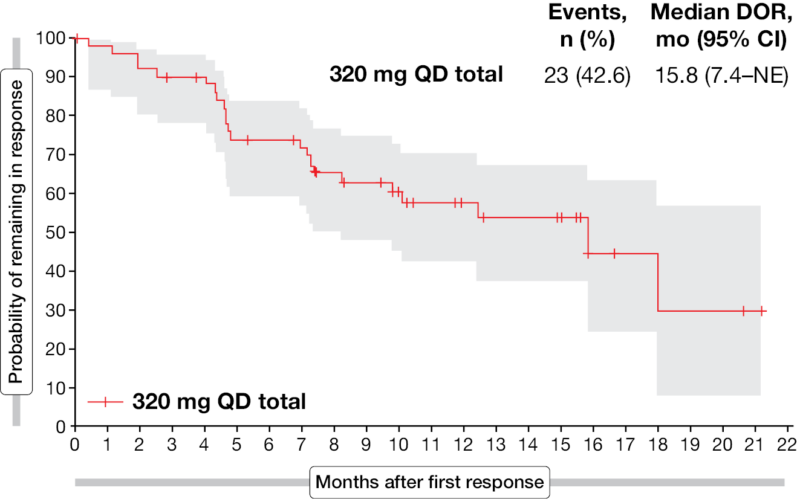
Figure 6: Probability of remaining in response for patients with partial and complete responses in the BGB-11417-201 clinical trial. CI, confidence interval; DOR, duration of response; NE, not evaluable; QD, once daily.
Resistance to BTKi spurs evaluation of early-phase BTK degraders
Patients with CLL/SLL experience disease progression with BTKi, often due to resistance mutations in BTK [11]. BTK degraders are a new class of drugs that specifically block B-cell receptor signaling by promoting proteasome-mediated degradation of both wild-type BTK and BTK-resistant mutations. Initial data from two new BTK degraders currently being tested in phase I/II trials in relapsed/refractory CLL/SLL were presented at ASH 2025 [12,13].
Inhye Ahn presented results from the CLL/SLL cohort of the CaDAnCe-101 (BGB-16673-101) study, an open-label, dose escalation/expansion study evaluating monotherapy with BGB-16673 in patients with B-cell malignancies [12].
Eligible patients must have confirmed R/R CLL/SLL with ≥2 prior therapies, including a covalent BTK inhibitor (cBTKi), if approved for their disease. In total, 68 CLL/SLL patients were treated with the drug at a dose between 50 and 600 mg once daily orally. Patients were heavily pre-treated, with a median of 4 prior lines of therapy (range, 2-10), and almost 90% discontinued prior BTKi due to disease progression. After a median treatment duration of 13.6 months, TEAEs occurred in 95.6% of patients, most commonly fatigue (36.8%) and contusion (bruising; 30.9%). Grade ≥3 TEAEs occurred in 61.8% of patients, primarily neutropenia (25%) and pneumonia (12%). Three patients discontinued treatment due to treatment-related TEAEs, and no treatment-related deaths were reported.
The ORR was 85.3%, with most patients achieving PR (72.1%) or partial response with lymphocytosis (PR-L; 10.3%). The intermediate dose of 200 mg showed the highest ORR (94.4%). Significant antitumor activity was observed, regardless of BTK mutation status and the number of prior lines of therapy. ORR was 75% in patients with triple exposure to covalent BTK, non-covalent BTK, and BCL2 inhibitors. After a median study follow-up of 19.8 months, the 18-month PFS rate of 65.9% indicating sustained disease control. Based on these results, the 200 mg dose was selected as the recommended dose for the expansion study. BGB-16673 is currently being evaluated in ongoing phase II and phase III studies in R/R CLL.
Zulfa Omer presented updated findings from the first-in-human trial (NX-5948-301) of a novel BTK degrader, bexobrutideg, in patients with relapsed/refractory B-cell malignancies [13]. The phase Ia/1b study included 126 heavily pretreated CLL/SLL patients treated with a range of bexobrutideg doses (50-600 mg). After a median follow-up of 19 months (phase Ia, 9.8 months in phase Ib), bexobrutideg was well tolerated with no dose-limiting toxicities. The most common adverse events were purpura/contusion, neutropenia (grade ≥3: 23.7%), fatigue, and diarrhea.
The ORR was 83% (CR-rate of 4.3%), with rapid responses (median 1.9 months) and sustained remissions (median PFS: 22.1 months) across all doses, including those in difficult-to-treat subgroups with baseline BTK mutations, high-risk molecular features and central nervous system involvement. In the Phase Ib randomized cohort of the trial (200 mg vs. 600 mg), higher ORR and superior PFS were observed at the 600 mg bexobrutideg dose, supporting its selection as the recommended phase 2 dose. Bexobrutideg will be evaluated in the ongoing pivotal phase II DAYBreak CLL-201 and planned phase III DAYBreak CLL-306 trials.
These early findings from two new BTK degraders showed a manageable safety profile and rapid, profound remissions in heavily pretreated CLL groups, particularly those resistant to BCL2i or covalent/non-covalent BTKi, offering hope for new treatment options for CLL/SLL patients

Figure 7: Summary of all grade TEAEs in ≥10% of all patients from CaDAnCe-101. TEAE, treatment-emergent adverse event.

Figure 8: TEAEs in ≥10% in Phase 1a/b NX-5948-301 comparing 600 mg group vs all patients. TEAE, treatment-emergent adverse event.
REFERENCES
- Al-Sawaf O, Stumpf J, Zhang C, et al. Fixed-duration versus continuous targeted treatment for previously untreated chronic lymphocytic leukemia:
Results from the randomized CLL17 trial. Blood 2025;146:1. https://doi.org/10.1182/blood-2025-1. - Al-Sawaf O, Stumpf J, Zhang C, et al. Fixed-Duration versus Continuous Treatment for Chronic Lymphocytic Leukemia. N Engl J Med 2025. https://doi.org/10.1056/NEJMoa2515458.
- Jurczak W, Kwiatek M, Czyz J, et al. Pirtobrutinib vs bendamustine plus rituximab (BR) in patients with CLL/SLL: First results from a randomized phase III study Examining a non-covalent BTK inhibitor in untreated patients. Blood 2025;146:LBA-3. https://doi.org/10.1182/blood-2025-LBA-3.
- Jurczak W, Kwiatek M, Czyz J, et al. BRUIN CLL-313: Randomized Phase III Trial of Pirtobrutinib Versus Bendamustine Plus Rituximab in Untreated Patients With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. J Clin Oncol 2025;0:JCO-25-02380. https://doi.org/10.1200/JCO-25-02380.
- Tam C, Munir T, Robak T, et al. Sustained efficacy of zanubrutinib (zanu) vs bendamustine + rituximab (BR) in treatment (tx)-naive chronic lymphocytic leukemia/small lymphocytic lymphoma (TN SLL/CLL) and continued favorable survival in non-randomized patients (pts) with del(17p): 6-year follow-up in the phase 3 SEQUOIA study. Blood 2025;146:2129. https://doi.org/10.1182/blood-2025-2129.
- Brown J, Victor T, Wu A, et al. Symptom-based progression-free survival (S-PFS) as a clinically relevant and patient-centric endpoint in chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL): Results from the ALPINE trial. Blood 2025;146:711. https://doi.org/10.1182/blood-2025-711.
- Eichhorst B, Niemann CU, Kater AP, et al. First-Line Venetoclax Combinations in Chronic Lymphocytic Leukemia. N Engl J Med 2023;388:1739–54. https://doi.org/10.1056/NEJMoa2213093.
- Liu J, Li S, Wang Q, et al. Sonrotoclax overcomes BCL2 G101V mutation–induced venetoclax resistance in preclinical models of hematologic malignancy. Blood 2024;143:1825–36. https://doi.org/10.1182/blood.2023019706.
- Hoffmann M, Ma S, Eradat H, et al. MRD-guided therapy of sonrotoclax (BGB-11417) + obinutuzumab (O) in patients with treatment-naive CLL: Initial results from an ongoing phase 1/1b study, BGB-11417-101. Blood 2025;146:793. https://doi.org/10.1182/blood-2025-793.
- Wang M, Song Y, Hermine O, et al. Sonrotoclax (BGB-11417) monotherapy in patients with Relapsed/Refractory (R/R) Mantle Cell Lymphoma (MCL) previously treated with a bruton tyrosine kinase (BTK) inhibitor: Early results from A phase 1/2 study. Blood 2025;146:663–663. https://doi.org/10.1182/blood-2025-663.
- Wang E, Mi X, Thompson MC, et al. Mechanisms of Resistance to Noncovalent Bruton’s Tyrosine Kinase Inhibitors. N Engl J Med 2022;386:735–43. https://doi.org/10.1056/NEJMoa2114110.
- Ahn I, Parrondo R, Thompson M, et al. Updated efficacy and safety results of the Bruton tyrosine kinase (BTK) degrader BGB-16673 in patients with relapsed/refractory chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) from the ongoing phase 1 CaDAnCe-101 study. Blood 2025;146:85. https://doi.org/10.1182/blood-2025-85.
- Omer Z, Danilov A, Forconi F, et al. Bexobrutideg (NX-5948), a novel Bruton’s tyrosine kinase (BTK) degrader, demonstrates rapid and durable clinical responses in Relapsed/Refractory chronic lymphocytic leukemia (CLL): New and updated findings from an ongoing Phase 1a/b trial. Blood 2025;146:86–86. https://doi.org/10.1182/blood-2025-86.
© 2026 Springer-Verlag GmbH, Impressum
More posts
A PARADIGM shift in newly diagnosed fit AML
Standard initial treatment for acute myeloid leukemia (AML) patients varies based on age and fitness. Typically, younger and fit patients, under 65 years old, receive intensive induction chemotherapy (IC), commonly known as the “7+3” regimen, which consists of cytarabine and an anthracycline, followed by consolidation therapy, allogeneic stem-cell transplantation (HCT), or a combination of both.
New BTK modalities in B-cell malignancies
Targeted agents such as Bruton tyrosine kinase inhibitor (BTKi; e.g., ibrutinib) and B-cell lymphoma-2 inhibitors (BCL2i) have emerged for the treatment of Chronic Lymphocytic Leukemia (CLL).
Deepening and extending response to treatment in Multiple Myeloma
The open-label, randomized phase III trial DREAMM-7 compared the safety and efficacy of two combination treatments, BVd (Belantamab-Mafodotin, Bortezomib, dexamethasone) and DVd (Daratumumab + Vd) in patients with refractory and relapsing Multiple Myeloma (R/R MM) who have received ≥ 1 line of treatment (LOT).
Preface – ASH 2025
Out of the 8,200 abstracts accepted for the ASH 2025 annual congress, we highlight several key abstracts that discuss targeted treatment strategies for lymphoid and myeloid malignancies, especially the high-impact ones showcased in the late-breaking abstract and plenary sessions.