EGFR-mutation-positive NSCLC: expanding the data pool for established treatment options
Subgroup analyses of LUX-Lung 3 and 6
Non–small-cell lung cancer (NSCLC) with activating epidermal growth factor receptor (EGFR) mutations represents a defined molecular subset of lung cancer that can be targeted with EGFR tyrosine kinase inhibitor (TKI) therapies. Erlotinib, gefitinib and afatinib have been approved as first-line treatment options for EGFR-mutation-positive NSCLC. While the first-generation TKIs erlotinib and gefitinib work by reversibly inhibiting EGFR, the second-generation TKI afatinib acts as an ErbB family blocker by irreversibly inhibiting a broader range of signalling cascades. The efficacy of first-line afatinib was demonstrated by the two large phase III trials LUX-Lung 3 and 6, which consistently showed superior progression-free survival (PFS) with afatinib as compared to standard platinum-doublet chemotherapy [1, 2]. Also, overall survival (OS) was significantly improved in patients with deletion 19 mutations[3].
According to subgroup analyses of the LUX-Lung 3 and 6 trials presented at the ESMO Asia Congress, the OS findings were consistent across Asian, non-Asian and Japanese patients [4]. In all ethnic subgroups, significant OS improvements of 10 to 15 months were seen for patients with deletion 19 mutations (Table), while median OS did not differ significantly between the treatment arms in those harbouring the L858R mutation.
Likewise, further subgroup analyses of LUX-Lung 3 and 6 established similar efficacies of afatinib treatment in patients aged ≥ 65 years and in the general study population [5]. In LUX-Lung 3, elderly patients experienced significant OS improvement when deletion 19 mutation was present (median OS, 41.5 vs. 14.3 months for afatinib and chemotherapy, respectively; hazard ratio [HR], 0.39; p = 0.0073). For LUX-Lung 6, these results were in favour of afatinib as well (34.1 vs. 21.1 months), but not significantly so. The adverse event (AE) profile was comparable to that of the overall population. Based on these results, afatinib can also be considered for patients aged ≥ 65 years with advanced EGFR-mutation-positive NSCLC.
LUX-Lung 7: afatinib versus gefitinib in the first-line setting
Head-to-head comparisons of first-line TKIs that provide guidance for clinical decision making have been lacking to date. The global, randomised, phase IIB LUX-Lung 7 trial compared afatinib with gefitinib for untreated patients with IIIB/IV adenocarcinoma of the lung and EGFR mutation (deletion 19 and/or L858R) [6]. At 64 centres in 13 countries, including North America, Europe, Asia and Australia, participants were randomised to either afatinib 40 mg once daily (n = 160) or gefinitib 250 mg once daily (n = 159). Treatment beyond progression was allowed if it was deemed appropriate by the investigator. LUX-Lung 7 had three co-primary endpoints: PFS, time to treatment failure (TTF), and OS. The primary analysis of the trial was presented at ESMO Asia 2015.
For the key primary endpoint of PFS (by independent review), the results were significantly in favour of afatinib (median PFS, 11.0 vs. 10.9 months; HR, 0.73; p = 0.0165; Figure 1). At 18 and 24 months, marked differences between the two treatment arms emerged. The afatinib-related PFS advantage was seen across the subgroups, and it was not affected by mutation type (deletion 19 vs. L858R mutation) or other factors.
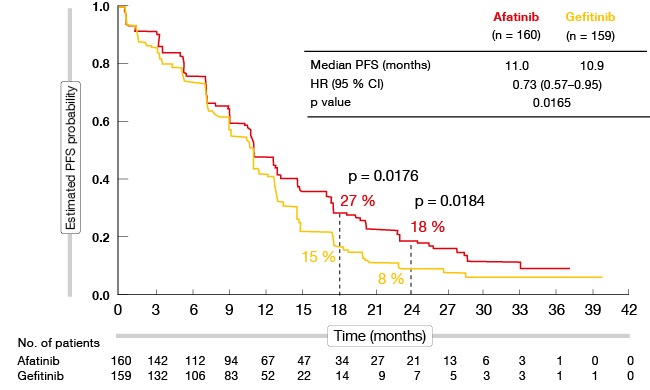
Figure 1: PFS benefit of afatinib as compared to gefitinib in LUX-Lung 7
With respect to the second co-primary endpoint of TTF, the analysis showed that afatinib-treated patients tended to remain on treatment for longer periods of time (median, 13.7 vs. 11.5 months; HR, 0.73; p = 0.0073). This difference is in agreement with the PFS gain. The OS data are still immature and should become available in the course of 2016.
Response and tolerability outcomes in LUX-Lung 7
Across the afatinib and gefitinib treatment arms, objective responses occurred in 70 % vs. 56 %, respectively (p = 0.0083). Also, the median duration of response was longer in the afatinib group than for gefitinib (10.1 vs. 8.4 months). In patients with deletion 19 mutation, afatinib therapy provided marked benefits for PFS (HR, 0.76), response rates (73 % vs. 66 %), and tumour shrinkage. These benefits, however, were even greater in patients with L858R mutation (PFS: HR, 0.71; response rates, 66 % vs. 42 %).
Also, the results confirm the general manageability of the side effects of these drugs. The AEs were predictable and manageable and did not deviate from the known toxicity profiles in terms of frequency or severity. Even though most of the patients experienced some type of AE, the rates of drug discontinuation due to AEs were identical and low, at 6.3 % in both arms. Diarrhoea was the predominant reason for drug discontinuation in the afatinib group, followed by fatigue and toxic skin eruptions. In the gefitinib arm, the most common causes of discontinuation were transaminase elevations and interstitial lung disease. Overall, LUX-Lung 7 confirms the benefits of irreversible ErbB blockade with afatinib compared to reversible EGFR inhibition with gefitinib in the treatment of EGFR-mutation-positive NSCLC. These findings can be used to support treatment decisions between first-line TKIs in clinical practice.
Update of LUX-Lung 8
Whereas LUX-Lung 7 compared afatinib and gefitinib in the first-line setting in patients with EGFR-positive adenocarcinomas, the global, randomised, open-label, phase III LUX-Lung 8 trial applied the afatinib versus erlotinib comparison to second-line patients with squamous-cell carcinomas, independent of mutation status. According to the primary analysis, significant improvements in PFS and OS have been achieved with afatinib over erlotinib [7].
At the ESMO Asia Congress, the primary OS analysis after 632 deaths was reported, as well as updated PFS results and exploratory tumour genetic findings [8]. OS was significantly improved with afatinib compared to erlotinib (median, 7.9 vs. 6.8 months; HR, 0.81; p = 0.0077; Figure 2). The significant PFS advantage remained, with median results of 2.6 vs. 1.9 months (HR, 0.81; p = 0.0103). Molecular aberrations occurred with incidences similar to those previously observed by The Cancer Genome Atlas Research Network. TP53, LRP1B, MLL2 SVs, SOX2, KLHL6, PIK3CA and MAP3K13 CNAs counted among the most frequent aberrations. The afatinib-related benefit was seen across all of the clinical and molecular subgroups. There was no predictive association between genetic alterations and OS or PFS. These data support afatinib as the TKI of choice in second-line treatment of patients with squamous-cell carcinoma of the lung.
Figure 2: Improvement of OS with afatinib as compared to erlotinib in LUX-Lung 8
Biomarker findings for afatinib
The efficacy of gefitinib and erlotinib monotherapies can be predicted by the early development of skin rash. To establish whether this relationship also applies to afatinib treatment, Bessho et al. retrospectively assessed 49 consecutive patients with EGFR-mutant NSCLC who received afatinib monotherapy between 2009 and 2015 [9]. Ten percent of the patients developed skin rash grade ≥ 2 within the first week. Multivariate analysis revealed a trend for increased responses with the occurrence of grade ≥ 2 early skin rash (p = 0.071).
Studies hint at the usefulness of circulating free DNA (cfDNA) for the detection and monitoring of EGFR mutations. Iwama et al. provided prospective data for afatinib by evaluating tumour samples and blood samples from 35 afatinib-treated patients, with the aim of investigating the usefulness of non-invasive liquid biopsies [10]. Samples were taken before, during, and after treatment.
The treatment provided a response rate of 77.1 %. Disease control was achieved in 88.6 %, and median PFS had not been reached at the time of analysis. The detection rate of active mutations in cfDNA before the administration of afatinib was high, at 59.4 % for Scorpion-ARMS, 81.3 % for digital polymerase chain reaction, and 75.0 % for next-generation sequencing. After the start of treatment, the concentrations of L858R-positive alleles in cfDNA dropped sharply until week 4, and then stayed at low levels in the patients who did not progress. This was also true for the concentrations of exon-19-deletion-positive alleles. Overall, active mutations were detected in cfDNA to a much greater extent before treatment and after progression than during treatment (Figure 3). The quantitative changes of active mutations thus reflected the clinical course of the disease.
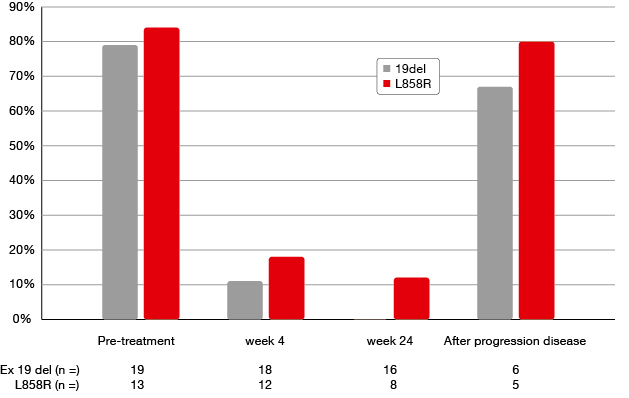
Figure 3: Differences in the detection of active mutations in cfDNA before, during and after treatment with afatinib
Addition of bevacizumab to erlotinib in specific circumstances
Anti-EGFR TKI monotherapy might not be sufficient in patients with certain clinical factors. A potential strategy to improve the efficacy of treatment is the combination with anti-vascular endothelial growth factor agents. The open-label, randomised, multicentre, phase II JO25567 trial demonstrated a PFS advantage of erlotinib plus bevacizumab, as compared to erlotinib alone, in chemotherapy-naïve patients with non-squamous, EGFR-mutation-positive, stage IIIB/IV NSCLC [11]. For the entire cohort, median PFS was 16.0 versus 9.7 months with erlotinib plus bevacizumab and erlotinib monotherapy, respectively (HR, 0.54; p = 0.0015).
A subgroup analysis of JO25567 that was presented at the ESMO Asia Congress showed consistent benefit for the addition of bevacizumab to erlotinib regardless of patient characteristics [12]. At the same time, some factors appeared to be associated with shorter PFS in the monotherapy arm. This was especially the case for baseline pleural and/or cardiac effusion (PCE). In patients with PCE, those who received erlotinib alone had a median PFS of only 5.7 months, compared to 15.4 months in the combination group (HR, 0.45; Figure 4). This difference was much smaller in patients without PCE (16.4 vs. 11.1 months, for erlotinib plus bevacizumab and erlotinib, respectively; HR, 0.62).
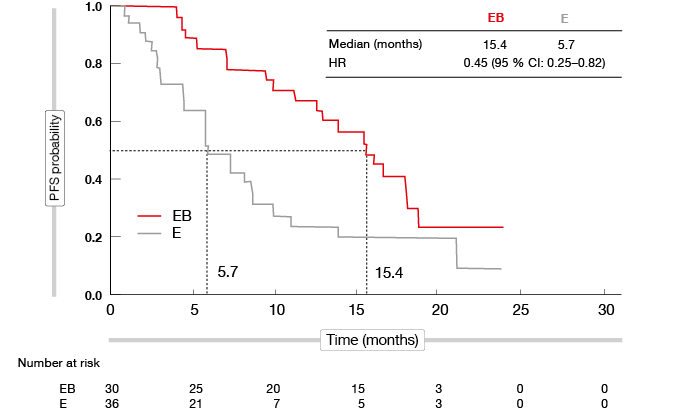
Figure 4: Marked reduction in the risk of progression and death with erlotinib plus bevacizumab compared to erlotinib alone in patients with pleural and/or cardiac effusion
Objective response rates were approximately 70 % in the combination arm, regardless of whether PCE was present or not. On the other hand, in the monotherapy arm, patients with PCE had lower response rates (56 %) than those without (71 %). Progression of baseline PCE was more frequent in the monotherapy arm (30.6 %) than in the combination arm (16.7 %), which indicated improved control with the addition of bevacizumab. No new safety signals were observed, regardless of the presence of baseline PCE.
REFERENCES
- Sequist LV et al., Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol 2013; 31: 3327-3334
- Wu YL et al., Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non–small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised phase 3 trial. Lancet Oncol 2014; 15: 213-222
- Yang JC et al., Afatinib versus cisplatin-based chemotherapy for EGFR-mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): analysis of overall survival data from two randomised, phase 3 trials. Lancet Oncol 2015; 16: 141-151
- Wu YL et al., Overall survival with afatinib versus chemotherapy in patients with NSCLC harbouring common EGFR mutations: subgroup analyses by race/ ethnicity in LUX-Lung 3 and LUX-Lung 6. ESMO Asia 2015, abstract 445P
- Wu YL et al., Afatinib versus chemotherapy for EGFR mutation-positive NSCLC patients aged ≥ 65 years: subgroup analyses of LUX-Lung 3 and LUX-Lung 6. ESMO Asia 2015, abstract 446P
- Park K et al., Afatinib versus gefitinib as first-line treatment for patients with advanced non-small cell lung cancer harbouring activating EGFR mutations: LUX-Lung 7. ESMO Asia 2015, abstract LBA2_PR
- Soria J-C et al., Afatinib versus erlotinib as second-line treatment of patients with advanced squamous cell carcinoma of the lung (LUX-Lung 8): an open-label randomised controlled phase 3 trial. Lancet Oncol 2015; 16: 897-907
- Park K et al., Phase III trial of afatinib versus erlotinib in patients with squamous cell carcinoma of the lung (LUX-Lung 8): EGFR molecular aberrations and survival outcomes. ESMO Asia 2015, abstract 443P
- Bessho A et al., Development of skin rash within the first week is a potential surrogate marker of effect in afatinib for EGFR mutant NSCLC: Okayama Lung Cancer Study Group experience. ESMO Asia 2015, abstract 453P
- Iwama O et al., A multicentre prospective biomarker study in afatinib-treated patients with EGFR-mutation-positive non–small-cell lung cancer. ESMO Asia 2015, abstract 484PD
- Seto T et al., Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non–small-cell lung cancer harbouring EGFR mutations (JO25567): an open-label, randomised, multicentre, phase 2 study. Lancet Oncol 2014; 15(11): 1236-1244
- Hosomi Y et al., Erlotinib plus bevacizumab versus erlotinib alone as first-line treatment for advanced non-squamous non-small-cell lung cancer with activating EGFR mutation: JO25567 exploratory subgroup analysis. ESMO Asia 2015, abstract 420O
More posts
Immunotherapy: management of toxicity
The basis underlying the toxicities of immune checkpoint inhibitors is their promotion of T-cell activity in a physiological manner. “The amplification of the immune system results in autoimmunity,” explained Ross Soo, MD, FRACP, National University Cancer Institute, Singapore. Common AEs include fatigue, anorexia and arthralgia. Terms that denote immune-related adverse events (irAEs) typically end in -itis or -opathy.
PD-L1 expression is a nightmare in terms of complexity
here are two issues that are tied to the topic of biomarkers in immunotherapies. First, all attempts to define biomarkers have focused primarily on response as a marker of efficacy. We have to be aware, however, that immunotherapies are not targeted therapies, and fast tumor shrinkage is not necessarily observed with this kind of treatment. The efficacy of an immunotherapy is defined by long-lasting tumor stabilization.
Immunotherapy: anti-tumour activity despite extensive pretreatment
The anti-PD-1-antibodies pembrolizumab and nivolumab have been shown to be active in lung cancer. Pembrolizumab is a high-affinity, humanised, monoclonal IgG4κ antibody against PD-1 that prevents the interaction of the receptor with PD-L1 and PD-L2. The KEYNOTE-001 trial demonstrated significant anti-tumour activity of pembrolizumab in advanced NSCLC, with improved outcomes in terms of PD-L1 Tumor Proportion Scores (TPS) ≥ 50 %.
Risks and chances in patients with oligometastatic disease
Against the background of improved systemic therapies, there are rising expectations with regard to the potential cure of NSCLC patients who have a limited number of haematogeneous metastases. “Most studies define oligometastasis as one to three, or one to five lesions,” explained Suresh Senan, MRCP, FRCR, PhD, VU University Medical Centre, Amsterdam, The Netherlands.
Disease progression on EGFR TKI therapy: what to do after erlotinib, gefitinib and afatinib?
The most common mechanism of acquired resistance is the T790M mutation within exon 20 of the EGFR gene (Figure 1). Indolent slow tumour growth typically occurs when this mutation emerges. “Repeated imaging may be necessary to identify progression,” explained Pasi A. Jänne, MD, PhD, Lowe Center for Thoracic Oncology, Dana Farber Cancer Institute, Boston, USA, during a symposium at the ESMO Asia Congress.
EGFR-mutation-positive NSCLC: expanding the data pool for established treatment options
Non–small-cell lung cancer (NSCLC) with activating epidermal growth factor receptor (EGFR) mutations represents a defined molecular subset of lung cancer that can be targeted with EGFR tyrosine kinase inhibitor (TKI) therapies. Erlotinib, gefitinib and afatinib have been approved as first-line treatment options for EGFR-mutation-positive NSCLC.