

Advances in PSMA-based immunotherapy in metastatic castration-resistant prostate cancer
Metastatic castration-resistant prostate cancer (mCRPC) has a very bad prognosis with most patients dying within two years of diagnosis [1]. Available therapies for mCRPC are often associated with poor tissue selectivity, and side effects including high systemic toxicity and drug resistance. Great progress has been made with the help of PSMA (prostate-specific membrane antigen), a glycoprotein highly expressed on the cell membrane of malignant prostate tumor cells, which constitutes an attractive therapeutic candidate for both diagnosis and treatment of mCRPC [2]. Briefly, PSMA-based immunotherapy specifically targets tissues expressing the protein, either the primary tumor or metastases. However, PSMA is expressed in normal tissues such as salivary glands, kidney, ovary, breast, the neo-vasculature of non-prostatic tumors and intestine, too, and high uptakes of radiopharmaceuticals might lead to dose-limiting toxicities [2-4].
ProstACT GLOBAL: a phase 3 study with 177Lu-DOTA-rosopatamab
TLX591 consists of the humanized monoclonal antibody rosopatamab (HuJ591), targeting an epitope of the extracellular domain of PSMA, conjugated to DOTA, a chelating agent (DOTA-HuJ591). This chelator conjugated antibody can be linked to different radioisotopes for diagnostic (89Zirconium) or therapeutic purposes (177Lutetium, 111Indium or 90Yttrium) [5, 6]. Rosopatamab has a high affinity for PSMA, its target epitope, and does not bind to complement [6]. So far, 177Lu-HuJ591 has been tested in more than 100 patients in four phase 1 and 2 studies with single as well as repeated and fractionated doses [5]. Rosapatamab has further been evaluated in combination with standard-of-care docetaxel in a phase 1 study including 15 patients with progressive mCRPC and showed preliminary encouraging efficacy [7]. During EANM 2023, Neel Patel presented the design of the ongoing ProstACT GLOBAL multinational, multicenter, randomized, controlled, open-label phase 3 study (NCT04876651) [8]. The efficacy and safety of 177Lu-DOTA-rosopatamab plus best standard of care (SoC), as compared to best SoC alone, is investigated in patients with progressive mCRPC despite previous treatment with a novel androgen-axis drug (NAAD). Patients considered eligible must present with a PSMA-positive disease and at least one metastatic site, as assessed by 68Gallium-PSMA-11 positron emission tomography/computerized tomography (68Ga-PSMA-11 PET/CT) scan, have received prior therapy with either enzalutamide or abiraterone plus prednisone, as well as prior taxane therapy unless they have refused it or are ineligible; patients must also present adequate hematological function as demonstrated by normal platelet count (≥ 150 x 109/L) and normal hemoglobin (≥ 10 g/dL).
The planned 387 patients will be randomized 2:1 to either two 14-days-apart single intravenous injections of 76 millicuries (mCi) each of 177Lu-DOTA-rosopatamab (equivalent to a 45 mCi/m2 dose in a standard 1.7 m2 individual) on top of best SoC, or best SoC alone. Stratification factors will be based on prior taxane therapy, prior NAAD setting (non-metastatic versus castration-sensitive), disease burden as defined by bone metastases number with a cut-off at 10, and visceral disease (or not).
The primary objective of ProstACT GLOBAL is the radiographic progression-free survival (rPFS); secondary endpoints further evaluate the 5-year overall survival (OS), the tumor objective response rate (ORR) and the time to symptomatic skeletal event (TTSSE), as well as the assessment of treatment-related adverse events (TRAEs).
The study is currently ongoing and will provide new insights into the benefits of combined radiotherapy and immunotherapy, in addition to efficient 68Ga-PSMA-11 PET/CT-base selection of patients with mCRPC.
Good tolerance to low dose 177Lu-PSMA-617 therapy
At this year’s EANM, Irene Marini presented preliminary results of IRST-185.03, an open-label, single-center, phase 2, prospective study (NCT03454750) evaluating the efficacy and toxicity of low-dose radiometabolic therapy with 177Lu-PSMA-617 in advanced mCRPC. The study enrollment started in April 2017 and closed in October 2022 [9]. The primary objective of the study was efficacy, as assessed by best biochemical response (BR) defined as a PSA reduction of at least 50 % versus baseline value. Secondary objectives encompassed safety, PFS and OS. Inclusion criteria comprised histologically confirmed progressive prostate cancer with metastases documented by 68Gallium-PSMA-11 PET/CT scan, adequate hematological organ function and ECOG score ≤ 2.
In total, 43 patients were included in the low-dosage (LD) group (3.7-4.4 GBq per cycle) and 99 patients in the high-dosage (HD) group (5.5 GBq per cycle) based on age (cut-off at 75 years), prior treatment with docetaxel and risk factors for toxicity. The median age was 70.2 years and median PSA value was 45.7 ng/mL at baseline. Overall, 90.1 % of patients had received prior treatment with abiraterone/enzalutamide and 62.7 % with docetaxel, while 29.6 % had been rechallenged with cabazitaxel or docetaxel. To note, 37.2 % of patients presented more than 20 bone metastatic lesions and 17.6 % had visceral metastases. Both groups received a median of four cycles (up to six) of 177Lu-PSMA-617, eight to twelve weeks apart, with concomitant mannitol intra-venous infusion for kidney protection and polyglutamate folate tablets orally for salivary glands protection [10].
After a median follow-up of 28.8 months, the PSA ≥50 % was achieved in 40.1 % of all patients; in more detail, a PSA reduction of ≥50 % was observed in 42.4 % patients in the HD group and in 34.9 % of patients in the LD group (Figure 1). Moreover, 51.4 % of the overall patient population showed a PSA reduction < 30 % or a PSA increase. The overall median PFS was 7.0 months (95 % CI: 5.5-7.6) and the 12-month PFS rate was 18.9 % (95 % CI: 12.2-26.6). The overall median OS was 16.8 months (95 % CI: 12.1-20.4) – 13.5 months (95 % CI: 8.4-19.2) in the LD group and 16.4 months (95 % CI: 12.1-25.3) in the HD group. The overall 12-month OS rate was 60.4 % (95 % CI: 50.5-68.6) – 51.1 % (95 % CI: 35.5-64.8) in the LD group and 64.9 % (95 % CI: 51.9-75.1) in the HD group.
The most common side effect was grade 1 anemia reported in 19 patients. Grade 3 toxicity was observed in seven patients, with five experiencing anemia and two experiencing renal toxicity. No grade 4 toxicity was reported.
These preliminary results show that 177Lu-PSMA-617, even at low doses, is efficient and well tolerated in selected, heavily pretreated mCRPC patients and justify further investigation of the minimum effective and non-toxic dosage of this radiometabolic therapy.
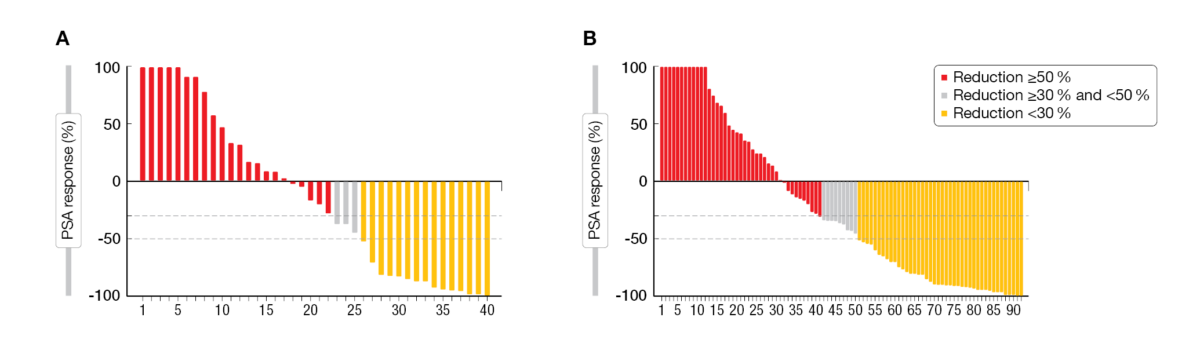
Figure 1: PSA response after (A) low-dose (3.7-4.4 GBq) and (B) high-dose (5.5 GBq) 177Lu-PSMA-617 treatment in mCRPC.
Swiss registry of mCRPC patients treated with 177Lu-PSMA-I&T
The objective of this prospective national registry is to assess the efficacy and the safety of 177Lu-PSMA-I&T (for imaging and therapy) therapying mCRPC implemented in daily clinical practice in Switzerland. Between February 2021 and May 2023, eight sites enrolled 246 patients with mCRPC, defined by PSMA-positivity, who failed or were unfit for chemotherapy, and had a progressive disease despite androgen-signaling inhibition therapy. During last year’s EANM, Nicolas Guillaume already presented preliminary safety (primary endpoint) and efficacy (key secondary endpoint) data from 107 patients receiving 7 GBq of 177Lu-PSMA-I&T every six weeks [11]. This year, Alin Chirindel presented an update on 147 evaluable patients [12]; a follow-up is planned until May 2024.
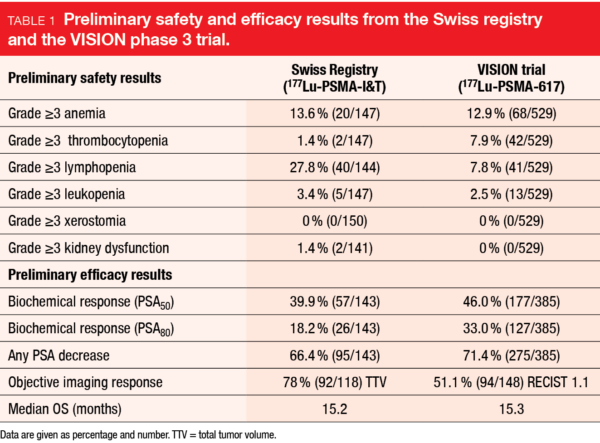
The enrolled patients had a median age of 75 years, a median baseline PSA of 72 ng/ml and metastases mostly in bones (95 % of patients) and/or lymph nodes (77 %). In the prior phase 3 VISION trial (NCT03511664), 50 % of patients had lymph node metastases and 21 % had metastases in soft tissues, compared to 30 % in the Swiss registry [13]. In total, 70 % of patients had a Gleason score between eight and ten, 71 % had received previous chemotherapy (97 % in VISION) and 99 % had underwent androgen-signaling inhibition therapy or orchidectomy (100 % in VISION). Patients received a median of three treatment cycles (IQR: 2-5) with a median of 7.1 GBq 177Lu-PSMA (IQR: 6.5-7.5), while VISION patients received a median of five cycles (IQR: 1-6).
A biochemical response was observed in 58.1 % of patients, with PSA levels ≤80 % in 18.2 % and ≤50 % in 39.9 % of patients. An objective imaging response – as evaluated by the tumor total volume [14] – was observed in 78 % of patients. The median PSA response and the median OS (15.2 months) are in line with the efficacy parameters observed with 177Lu-PSMA-617 in the VISION trial (Table 1 and [13]).
Treatment related grade ≥3 adverse events (AEs), shown in Table 1, include lymphopenia (27.8 %), anemia (13.6 %), leukopenia (3.4 %), kidney dysfunction (1.4 %) and thrombocytopenia (1.4 %).
The preliminary Swiss registry radioligand therapy data show that 177Lu-PSMA-I&T has a good safety profile and is efficient in mCRPC patients in a real-life setting.
Combined therapy with 225Ac-PSMA-617 and 177Lu-PSMA
Treatment options in patients with mCRPC after failure of guideline-conform or 177Lu-PSMA-radioligand therapies are very limited [15]. While 225Ac-PSMA-617-targeted alpha therapy (TAT) has demonstrated promising results in these patients, its associated adverse effects could substantially affect the quality of life of these patients [16]. A combination treatment regimen with 177Lu-PSMA and reduced 225Ac-TAT may improve tolerability, while maintaining an acceptable antitumor activity. At EANM 2023, Gabriel T. Sheikh presented the study outcomes in terms of response and adverse events in patients receiving different combinations of 225Ac-TAT/177Lu-PSMA-I&T (ALCT) [17].
A total of 22 mCRPC patients who failed previous guideline-based and/or 177Lu-PSMA-radioligand therapy were treated with ALCT: ten patients (Group 1) received 4 MBq 225Ac and 4000 MBq 177Lu, three patients (Group 2) received 6 MBq 225Ac and 1000 or 2000 MBq 177Lu, and nine patients (Group 3) received 8 MBq 225Ac and 1000 MBq 177Lu per therapy cycle. Clinical parameters (PSA, alkaline phosphatase, lactate dehydrogenase, hemoglobin, leukocyte count, thrombocyte count, creatinine) and imaging parameters from 18F-PSMA-PET/CT (Tumor Total Volume, SUVmax, SUVmean) were collected at baseline and after two cycles of therapy. AEs were evaluated according to CTCAE v5.0 and 18F-PSMA-PET/CT according to RECIP 1.0 (response evaluation criteria in PSMA PET/CT, [18]).
Regarding the efficacy of the three ALCT combinations, as evaluated by either clinical or imaging parameters, there was no statistically significant difference between the groups. AEs in Group 1, 2 and 3 after two cycles of ALCT included anemia in 20 %, 0 % and 33 %; thrombocytopenia in 10 %, 0 % and 0 %; leukopenia in 40 %, 33 % and 22 %; weight loss in 10 %, 0 % and 22 %, as well as xerostomia in 30 %, 33 % and 56 %, respectively. Overall, a higher 177Lu-activity was associated with bone marrow toxicity, while higher 225Ac-activity was more frequently associated xerostomia.
The three tested combinations of 225Ac-TAT/177Lu-PSMA-I&T showed an overall similar efficacy but different tolerability. Therefore, ALCT with low 225Ac-activity could be a favorable choice to minimize adverse effects on salivary glands. Nevertheless, it is imperative to closely monitor these patients for any changes in hematology parameters.
REFERENCES
- Lowrance WT et al. Castration-Resistant Prostate Cancer: AUA Guideline Amendment 2018. J Urol. 2018; 200(6): 1264-1272
- Sekhoacha M et al. Prostate cancer review: genetics, diagnosis, treatment options, and alternative approaches. Molecules. 2022; 27(17): 5730
- Wang F et al. Advances in PSMA-targeted therapy for prostate cancer. Prostate Cancer Prostatic Dis. 2022; 25(1): 11-26
- Langbein T et al. Salivary Gland Toxicity of PSMA-Targeted Radioligand Therapy with 177Lu-PSMA and Combined 225Ac- and 177Lu-Labeled PSMA Ligands (TANDEM-PRLT) in Advanced Prostate Cancer: A Single-Center Systematic Investigation. Diagnostics (Basel). 2022; 12(8): 1926
- Niaz MO et al. Review of lutetium-177-labeled anti-prostate-specific membrane antigen monoclonal antibody J591 for the treatment of metastatic castration-resistant prostate cancer. Cureus. 2020; 12(2): e7107
- Sartor O et Baghian A. Prostate specific membrane antigen binding radiopharmaceuticals: Current data and new concepts. Front Med (Lausanne). 2022; 9:1060922
- Batra JS et al. Phase I trial of docetaxel plus lutetium-177-labeled anti-prostate-specific membrane antigen monoclonal antibody J591 (177Lu-J591) for metastatic castration-resistant prostate cancer. Urol Oncol. 2020; 38(11): 848.e9-848.e16
- Patel N et al. ProstACT GLOBAL: a phase 3 study of 177Lu-DOTA-rosopatamab (TLX591) with and without the best standard of care for patients with PSMA expressing metastatic castration-resistant prostate cancer progressing despite prior treatment with a novel androgen axis drug. EANM 2023 (Oral abstract OP-718)
- Marini I et al. 177Lu-PSMA-617 therapy in advanced mCRPC patients: preliminary results of the phase 2 prospective trial IRST-185.03. EANM 2023 (Oral abstract OP-723)
- Paganelli G et al. Dosimetry and safety of 177Lu PSMA-617 along with polyglutamate parotid gland protector: preliminary results in metastatic castration-resistant prostate cancer patients. Eur J Nucl Med Mol Imaging. 2020; 47(13): 3008-3017
- Nicolas G et al. Safety and efficacy of PSMA targeted radionuclide therapy with 177Lu-ITG-PSMA-1 in metastatic castration resistant prostate cancer patients: preliminary results of a Swiss wide prospective multicentre registry study. EANM 2022 (Oral abstract OP-381)
- Chirindel A et al. Safety and efficacy of PSMA-targeted radionuclide therapy with 177Lu-ITG-PSMA-1 in metastatic castration resistant prostate cancer patients: Update on the prospective, multicenter, Swiss registry study. EANM 2023 (Oral abstract OP-716)
- Sartor O et al. VISION investigators. Lutetium-177-PSMA-617 for metastatic castration-resistant prostate cancer. N Engl J Med. 2021; 385(12): 1091-1103
- John N et al. 177Lu-PSMA SPECT Quantitation at 6 weeks (dose 2) predicts short progression-free survival for patients undergoing 177Lu-PSMA-I&T therapy. J Nucl Med. 2023; 64(3): 410-415
- Unterrainer LM et al. Total Tumor Volume on 18F-PSMA-1007 PET as Additional Imaging Biomarker in mCRPC Patients Undergoing PSMA-Targeted Alpha Therapy with 225Ac-PSMA-I&T. Biomedicines. 2022; 10(5): 946
- Ma J et al. Efficacy and safety of 225Ac-PSMA-617-targeted alpha therapy in metastatic castration-resistant prostate cancer: a systematic review and meta-analysis. Front Oncol. 2022; 12: 796657
- Sheikh G et al. Systematic evaluation of response and adverse events in mCRPC patients treated with different combinations of 225Ac/177Lu-PSMA-therapy. EANM 2023 (Oral abstract OP-717)
- Gafita A et al. Novel framework for treatment response evaluation using PSMA PET/CT in patients with metastatic castration-resistant prostate cancer (RECIP 1.0): an international multicenter study. J Nucl Med. 2022; 63(11): 1651-1658
© 2023 Springer-Verlag GmbH, Impressum
More posts
Theranostics: recent developments in neuroendocrine tumors
Theranostics: recent developments in neuroendocrine tumors 225Ac-DOTATATE daughter nuc