

Theranostics: recent developments in neuroendocrine tumors
225Ac-DOTATATE daughter nucleotide emissions
RYZ101 (225Ac-DOTATATE) is a first-in-class alpha-emitting radiopharmaceutical being developed for somatostatin receptor-2-expressing (SSTR2+) solid tumors [1]. The ongoing phase 1b/3 ACTION-1 trial (NCT05477576) is currently comparing RYZ101 with standard therapy in patients with well-differentiated gastroenteropancreatic neuroendocrine tumors (GEP-NETs) who have progressed after 177Lu-labelled somatostatin analogue (SSA) therapy. At EANM 2023, results from a dosimetry phase 1b sub-study in nine patients were presented [2].
The alpha decay series of 225AC-DOTATATE includes a total of four α-particle emissions (221Fr, 217At, 213Bi and 213Po) [3]. Thus, a key question of this study was whether the emissions of the 225Ac-DOTATATE daughter products are only found in the tumor lesions, or also affect other organs, causing off-target effects.
So far, 26 patients were enrolled in the phase 1b of the ACTION-1 trial. Seventeen patients were treated with 225Ac-DOTATATE at a dose of 120 kBq/kg (32 μCi/kg) administered intravenously for up to four cycles and observed for dose-limiting toxicities during Cycle 1 (8 weeks), whereas nine patients were enrolled in the dosimetry study. Dosimeter calculations were performed using SPECT/CT images acquired for Cycle 1 and Cycle 4 at 4 ± 1h, 24 ± 2h and 168 ± 24 h post-infusion. Two different energy windows were acquired to localize 221Fr and 213BI (218.2 keV ± 20 % and 440 keV ± 20 %). The activity was quantified in liver, kidneys, spleen, red bone marrow and tumors.
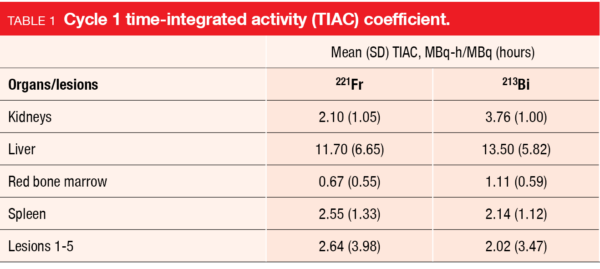
The results of the SPECT images of Cycle 1 showed that 221Fr and 213Bi mainly remained in the tumor, with only a small amount of free 213Bi reaching the kidneys. These results were confirmed by calculating the mean time-integrated activity coefficient (TIAC) (MBq-h/MBq) – see Table 1.
Assuming a similar dose distribution for each cycle, the mean estimated total absorbed dose of RYZ101 for the entire treatment period of four cycles (40.8 MBq [1,100 μCi]) is 11.7 Gy for tumors, 22.3 Gy for kidneys, 17.7 Gy for liver, 1.1 Gy for red bone marrow and 35.6 Gy for spleen, respectively.
These data implicate that imaging and obtaining quantitative information for dosimetry of 225Ac is feasible when 221Fr and 213Bi are directly and simultaneously imaged by SPECT/CT. For the first time, it has now been shown that the daughter products of 225Ac mostly stay with the delivery agent (DOTATATE) and only a minor fraction reaches the kidneys. Overall, these initial data suggest a favorable tumor-background profile for RYZ101 in SSTR+ GEP-NETs.
212Pb-VMT-α-NET: interim results from first in human pilot study
Alpha particles (such as 225Ac/212Pb) possess nearly 500 times the particle energy of beta particles (such as 177Lu). The high linear energy transfer radiation from alpha particles targets DNA inside the cell nuclei causing difficult to repair double-strand DNA breaks. [4, 5]
212Pb-VMT-α-NET is a modified peptide targeting the somatostatin receptor with improved pharmacokinetic properties used to treat SSTR2+ NETs. The VMT chelator efficiently binds both 212Pb and its daughter isotope 212Bi. Due to the short half-lives of the 212Bi daughter isotopes 208Tl (3 min) and 212Po (0.3 μs) and the strong chelating abilities of VMT-α-NET, the alpha particles of the decay series are mainly emitted in the targeted tissue. In tumor bearing mice, 212Pb-VMT-α-NET therapy was shown to be effective and well tolerated with a complete response rate of 100 % [6].
At EANM 2023, Dharmender Malik presented interim results from an open-label first in human pilot study evaluating the safety and efficacy of 212Pb-VMT-α-NET in patients with SSTR+ metastatic NETs who have failed at least one prior line of treatment [7]. Ten patients received 212Pb-VMT-α-NET therapy at a dose of 2.5 MBq/kg body weight 8-weekly for up to four cycles (with amino-acid co-infusion for renal protection). Of the included patients, three had gastrointestinal NETs, five pancreatic NETs and two a medullary thyroid carcinoma. Four patients had previously been treated with 117Lu-DOTATATE-peptide receptor radionuclide therapy (PRRT), and one person had also received 225Ac-DOTATATE-PRRT.
Patients who received one to four doses of 212Pb-VMT-α-NET showed a partial response already after the first administration; this effect increased with further doses of 212Pb-VMT-α-NET (Figure 1). A decrease in tumor size was observed in both the primary tumor and metastases. Moreover, quality of life benefits, as measured by the EORTC QLQ-GLNET21 score, showed an improvement in patients’ symptoms and quality of life after treatment with 212Pb-VMT-α-NET.
Treatment-related adverse events (TRAEs) were assessed 2-weekly and after four months of 212Pb-VMT-α-NET, therapy patients had stable values for hemoglobin level, total leucocyte count, platelet count and serum creatinine level. Most AEs were mild; they included grade I anemia, alopecia, or fatigue, which usually resolved within a week. No significant adverse effects on renal or hepatic function were reported. Currently, seven patients are still being treated with 212Pb-VMT-α-NET.
Overall, 212Pb-VMT-α-NET exhibited a favorable toxicity profile in NET patients, with high response rates at an initial dose. Upcoming survival data will provide further insights after a longer follow-up period.
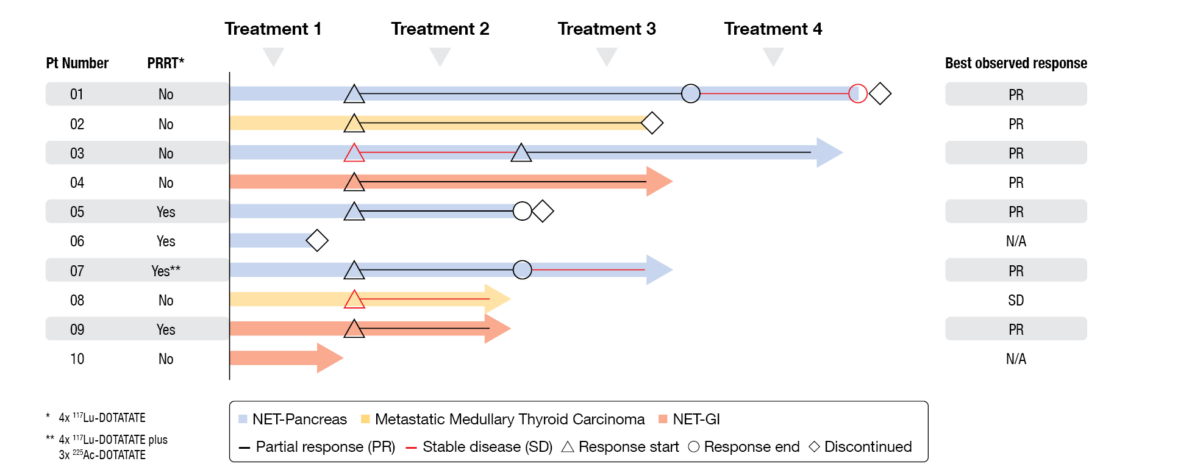
Figure 1: Interim results of patients with SSTR+ late-stage NETs treated with 212Pb-VMT-α-NET.
Personalized, dosimetry-based PRRT
PRRT is an effective treatment for patients with advanced SSTR expressing NETs [8]. However, there is still no consensus regarding the optimal PRRT treatment algorithm [9].
Thus, the multicenter, randomized phase III DUONEN trial (EUDRACT No: 2020-006068-99) aims to develop a dosimetry-based, personalized algorithm for tandem PRRT (mixed doses of [177Lu]Lu- and [90Y]Y-DOTATATE), and to evaluate the efficacy of personalized therapy with mixed doses of [177Lu]Lu- and [90Y]Y-DOTATATE compared to the treatment with [177Lu]Lu-DOTATATE in standard doses (7,400 MBq) [10].
In this study, adult patients with advanced, unresectable, well-differentiated (G1 and G2) NETs progressing on long-acting somatostatin analogues, are randomized into four groups: (A) 7,400 MBq [177Lu]Lu-DOTATATE per cycle; (B) [177Lu]Lu-DOTATATE plus [90Y]Y-DOTATATE starting at 3,700:1,850 MBq/MBq with [90Y]Y-DOTATATE activity being adjusted in Cycle 2 to Cycle 4 based on bone marrow and kidney dosimetry to achieve the highest radiation dose in tumor tissue; (C) [177Lu]Lu-DOTATATE plus 1,850 MBq [90Y]Y-DOTATATE with [177Lu]Lu-DOTATATE depending on dosimeter results; and (D) analogous to Arm A, followed by individualized dose adjustment based on dosimeter results. Moreover, PRRT dose in subsequent cycles will depend on individualized dosimetry results for critical organs (bone marrow, kidneys), with a kidney dose limit of 23 Gy and a bone marrow dose limit of 2 Gy (maximum of 0.5 Gy per cycle) for all PRRTs.
Treatment efficacy is assessed using morphological imaging (TK or MR) according to RECIST v1.1. The safety of PRRT is assessed by measuring the biochemical function of the kidneys and bone marrow.
At EANM 2023, Marta Opalińska presented data obtained from 21 patients (Arm A, n=5; Arm B, n= 6; Arm C, n= 4; Arm D, n=5; one patient awaiting randomization). A total of 39 PRRT cycles were administered, including 23 fixed doses (first doses or Arm A). In the 16 cycles scheduled for adjustment, the dose of radiopharmaceutical was increased in eleven patients, while being decreased in five. Four patients dropped-out due to disease progression or AEs. So far, both patients who underwent the first post-PRRT assessment according to RECIST v1.1 criteria achieved a partial response (Arm A) and a complete response (Arm B), respectively.
The preliminary results showed significant interindividual and intraindividual differences in absorbed radiation doses by critical organs, such as kidney and bone marrow, compared to the tumor tissue. This emphasizes the importance of personalized dosimetry allowing for PRRT dose adjustment (frequent increases) in subsequent treatment cycles, while maintaining the safety of the therapy.
Full-body longitudinal analysis of individual lesions in NET patients receiving PRRT
Baseline somatostatin receptor image features (SRIFs) correlate with peptide receptor radionuclide therapy (PRRT) outcomes in patients with metastatic neuroendocrine tumors (mNETs). Study data demonstrated that a reduced 68Ga-DOTATATE uptake in tumors following the first cycle of PRRT not only served as a predictor for the time to disease progression but was also linked to improved clinical symptoms among patients with well-differentiated NETs [11]. Nevertheless, the potential predictive value of longitudinal SRIFs obtained from each specific lesion has yet to be investigated. A recent study, presented by Victor Santoro-Fernandes at EANM 2023, addressed this question by examining the extent to which the longitudinal assessment of SRIFs enhances the prediction of progression-free survival (PFS) of mNET patients receiving PRRT [12].
Data from 68Ga-DOTATATE PET/CT scans of mNET patients – taken before (baseline) and after 177Lu-DOTATATE PRRT – were retrospectively analyzed. PFS was determined from medical records (median follow-up of 54 months) and used to stratify patients into poor and good responders. All lesions were contoured (lesion contouring), lesions were matched between imaging time points, and feature variation was calculated. Subsequently, lesion-level features were aggregated into patient-level features, which were further categorized into baseline and longitudinal sets.
In total, longitudinal images of 34 mNET patients were analyzed (mPFS, 20 months; min = 4, max = 54), with 18 patients classified as poor responders (PFS <31 months). Overall, a total of 2,521 lesions were identified (median: 38.5 per patient; min=5, max=381). The multivariate linear regression (MLR) model using longitudinal SRIFs resulted in more accurate PFS prediction (Figure 2) compared with single time-point baseline SRIFs reported by Haug AR et al. in 2010 [11] (RMSE, 13.5 vs. 14.1), and classification accuracy was also higher (AUROC, 0.81 vs. 0.74). Patient stratification was significant for longitudinal SRIFs but not for baseline SRIFs (log-rank test, p=0.003 vs. 0.06); this finding was further supported by the hazard ratios of 0.92 (95 % CI, 0.88-0.96; p<0.001) versus 0.96 (95 % CI, 0.92-1.00; p=0.04), respectively. While the MLR model outperformed all other machine learning models in predicting PFS, this may be attributed to the limited number of available training samples.
This work represents the first study to highlight the utility of full-body longitudinal SRIFs for predicting clinical outcomes. In mNET patients receiving PRRT, these results suggested that longitudinal SRIFs bring an additional benefit to PFS prediction compared to baseline SRIFs.
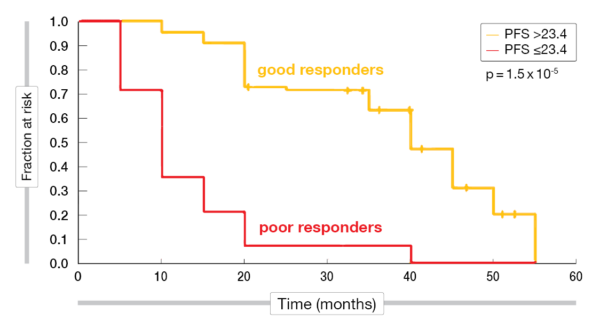
Figure 2: Multivariate linear regression using longitudinal SRIFs.
REFERENCES
- Rubira L et al. (225)Ac-labeled somatostatin analogs in the management of neuroendocrine tumors: from radiochemistry to clinic. Pharmaceutics 2023; 15(4): 1051
- Ulaner G et al. 225Ac-DOTATATE dosimetry results from part 1 of the ACTION-1 trial. EANM 2023 (Oral abstract OP-672)
- Shi M et al. Alpha-peptide receptor radionuclide therapy using actinium-225 labeled somatostatin receptor agonists and antagonists. Front Med (Lausanne) 2022; 9: 1034315
- Harris PE et al. The evolution of PRRT for the treatment of neuroendocrine tumors; what comes next? Front Endocrinol (Lausanne) 2022; 13: 941832
- Kunikowska J et al. Targeted alpha-emitter therapy of neuroendocrine tumors. Semin Nucl Med 2020; 50(2): 171-176
- Liu D. [203/212Pb]VMT-α-NET theranostic pair achieved complete response in SSTR2+ preclinical tumor model. https://www.isotopes.gov/sites/default/files/2022-10/203-212Pb%20Group%20panel%20meeting%20DOE_10042022%20%20-%20%20Read-Only.pdf. Letzter Zugang Oktober 2023
- Malik D et al. Early results of 212Pb-VMT-alpha-NET targeted therapy in metastatic gastro-entero-pancreatic neuroendocrine tumors: first in human clinical experience on safety and efficacy. EANM 2023 (Oral abstract OP-673)
- Hope TA et al. Neuroendocrine tumors and peptide receptor radionuclide therapy: when is the right time? J Clin Oncol 2022; 40(24): 2818-2829
- Adant S et al. Combination treatments to enhance peptide receptor radionuclide therapy of neuroendocrine tumours. Eur J Nucl Med Mol Imaging 2020; 47(4): 907-921
- Opalinska M et al. Personalized, dosimetry-based PRRT therapy in patients with neuroendocrine tumors using [177Lu]Lu-DOTATATE or [177Lu]Lu/[90Y]Y-DOTATATE mixture – the initial results
of DUONEN multicenter study. EANM 2023 (Oral abstract OP-675) - Haug AR et al. 68Ga-DOTATATE PET/CT for the early prediction of response to somatostatin receptor-mediated radionuclide therapy in patients with well-differentiated neuroendocrine tumors. J Nucl Med 2010; 51(9): 1349-1356
- Santoro-Fernandes V et al. Quantitative somatostatin receptor image assessment for survival prediction: a full-body, longitudinal, individual lesion analysis of neuroendocrine tumors in patients treated with peptide receptor radiation therapy. EANM 2023 (Oral abstract OP-676)
© 2023 Springer-Verlag GmbH, Impressum
More posts
Theranostics: recent developments in neuroendocrine tumors
Theranostics: recent developments in neuroendocrine tumors 225Ac-DOTATATE daughter nuc